Download
1 / 66
670 likes | 700 Vues
Learn about leprosy, a disease caused by Mycobacterium leprae, affecting the skin and nerves. Discover its signs, forms, and prevention methods.

E N D
LEPROSYCUTANEOUS TUBERCULOSISSARCOIDOSIS Özlem Akın, M.D. Yeditepe University Hospital Department of Dermatology
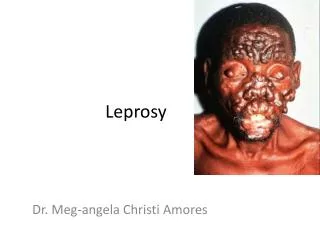
LEPROSY • a disease caused by the bacteria Mycobacterium leprae that causes damage to the skin and the peripheral nervous system • develops slowly (from six months to 40 years!) and results in skin lesions and deformities, most often affecting the cooler places on the body (for example, eyes, nose, earlobes, hands, feet, and testicles) • The skin lesions and deformities can be very disfiguring and are the reason that infected individuals were considered outcasts in many cultures • Although human-to-human transmission is the primary source of infection, three other species can carry and (rarely) transfer M. leprae to humans; chimpanzees, mangabey monkeys, and nine-banded armadillos • is termed a chronic granulomatous disease because it produces inflammatory nodules (granulomas) in the skin and nerves over time.
LEPROSY • is caused by Mycobacterium leprae, a rod-shaped bacillus that is an obligate intracellular (only grows inside of certain human and animal cells) bacterium • M. leprae is termed an "acid fast" bacterium because of its chemical characteristics • When special stains are used for microscopic analysis, it stains red on a blue background due to mycolic acid content in its cell walls • The Ziel-Nielsen stain is an example of the special staining techniques used to view the acid-fast organisms under the microscope • Currently, the organisms cannot be cultured on artificial media • The bacteria take an extremely long time to reproduce inside of cells (about 12-14 days as compared to minutes to hours for most bacteria) • The bacteria grow best at 80.9 F-86 F, so cooler areas of the body tend to develop the infection • The bacteria grow very well in the body's macrophages and Schwann cells (cells that cover and protect nerve axons)
LEPROSY • early signs and symptoms of leprosy are very subtle and occur slowly (usually over years) • Numbness and loss of temperature sensation are some of the first symptoms that patients experience • As the disease progresses, the sensation of touch, then pain, and eventually deep pressure are decreased or lost • Signs that occur, such as relatively painless ulcers, skin lesions of hypopigmented macules, and eye damage (dryness, reduced blinking) are experienced before the large ulcerations, loss of digits, and facial disfigurement develop • This long-time developing sequence of events begins and continues on the cooler areas of the body (for example, hands, feet, face, and knees)
LEPROSY • The forms of leprosy are based on the person's immune response to M. leprae. • A good immune response can produce the so-called tuberculoid form of the disease, with limited skin lesions and some asymmetric nerve involvement • A poor immune response can result in the lepromatous form, characterized by extensive skin and symmetric nerve involvement • Some patients may have aspects of both forms. Currently, two classification systems exist in the medical literature: • WHO system • Ridley-Jopling system • The 2009 WHO classifications are simply based on the number of skin lesions as follows: • Paucibacillary leprosy: skin lesions with no bacilli (M. leprae) seen in a skin smear • Multibacillary leprosy: skin lesions with bacilli (M. leprae) seen in a skin smear
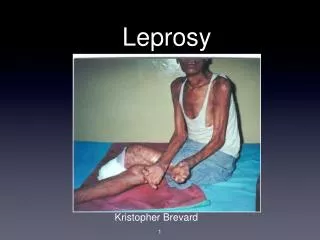
Lepromatous leprosy. diffuse infiltration of the face with leonine facies and madarosis.
The patient has madurosis, a saddle nose and blindness in the left eye
Borderline lepromatous leprosy. Multiple erythemous plaques are seen, some with central clearing.
Tuberculoid leprosy. Elevated border and central hypopigmentation.
LEPROSY • Researchers suggest that M. leprae are spread person to person by nasal secretions or droplets. They speculate that infected droplets reach other peoples' nasal passages and begin the infection there. • Some investigators suggest the infected droplets can infect others by entering breaks in the skin. M. leprae apparently cannot infect intact skin. • Rarely, humans get leprosy from the few animal species mentioned above. • Routes of transmission are still being researched for leprosy.
LEPROSY • Diagnosis: • Hypopigmented patches of skin or reddish skin patches with loss of sensation, thickened peripheral nerves, or both clinical findings together often comprise the clinical diagnosis • Skin smears or biopsy material that show acid-fast bacilli with the Ziel-Nelson stain or the Fite stain (biopsy) can diagnose multibacillary leprosy, or if bacteria are absent, diagnose paucibacillary leprosy
LEPROSY • Prevention: • Prevention of contact with droplets from nasal and other secretions from patients with untreated M. leprae infection currently is a way to avoid the disease. • Treatment of patients with appropriate antibiotics stops the person from spreading the disease. • People that live with individuals that have untreated leprosy are about eight times as likely to develop the disease, because investigators speculate that family members have close proximity to infectious droplets. • Leprosy is not hereditary. • Many people get exposed to leprosy throughout the world, but the disease in not highly contagious; researchers suggest that over 95% of exposures result in no disease. • There is no vaccine available to prevent leprosy. • Animals (chimpanzees, mangabey monkeys, and nine-banded armadillos) rarely transfer M. leprae to humans; nonetheless, handling such animals in the wild is not advised.
SARCOIDOSIS • characterized by noncaseating epithelioid granulomas that may affect any organ system • Although Jonathan Hutchinson described the first case in 1869, the etiology of the disease is still unknown • most commonly involves granuloma formation in the lungs • Other commonly involved organ systems include the lymph nodes (especially the intrathoracic nodes); the skin; the eyes; the liver; the heart; and the nervous, musculoskeletal, renal, and endocrine systems
SARCOIDOSIS • Pathophysiology • The etiology is unknown • increase in B-cell activity with hypergammaglobulinemia noted in about one half of patients and in nonspecific immune-complex formation • Reduced delayed-type hypersensitivity responses are also found in many patients • Cutaneous anergy to tuberculin intradermal testing occurs in two thirds of patients • Immune dysregulation has been theorized to be due to a persistent antigen of low virulence that is poorly cleared by the immune system, leading to a chronic T cell of the Th1 subtype response, which results in granuloma formation • Medications that increase the Th1 response, such as interferon, have been reported to trigger or exacerbate sarcoidosis • The gli -1 oncogene has been found to be highly expressed in persons with granulomatous skin diseases, including sarcoidosis.
SARCOIDOSIS • Proposed antigens fall into 3 categories that include infectious, environmental, and autoantigens. • The most common infectious agents implicated are Mycobacterium tuberculosis, Mycoplasma species, Corynebacteria species, spirochetes, atypical mycobacteria, Propionibacterium acnes, Borrelia burgdorferi, herpes simplex virus, hepatitis C virus, Epstein-Barr virus, cytomegalovirus, coxsackievirus, rubella virus, Histoplasma species, Cryptococcus species, coccidioidomycosis, and sporotrichosis. • Environmental antigens implicated include metals (eg, zirconium, aluminum, beryllium), organic dusts (eg, pine, pollen), and inorganic dusts (eg, clay, soil, talc). • Heat shock protein has also been implicated.
SARCOIDOSIS • Frequency • The prevalence is 1-40 cases per 100,000 population • In whites, the annual incidence is 10-14 cases per 100,000 population, whereas in African Americans, especially women, the annual incidence is much higher, at 35.5-64 cases per 100,000 population • affects people worldwide • found in every country and every race, although the incidence varies dramatically
SARCOIDOSIS • Mortality/Morbidity • The course of sarcoidosis is variable, ranging from self-limited acute disease to a chronic debilitating disease that may result in death • Spontaneous remissions occur in nearly two thirds of patients, but 10-30% of patients have a more chronic or progressive course. • The mortality rate is 1-6%. • can lead to death from severe involvement of lung parenchyma leading to pulmonary fibrosis and respiratory failure and from myocardial involvement leading to arrhythmias and cardiac failure. • Other causes of significant morbidity and mortality include CNS involvement, blindness, pulmonary hemorrhage, renal insufficiency, hypopituitarism, and liver disease.
SARCOIDOSIS • Adverse prognostic factors: • African American race • chronic cutaneous lesions • chronic uveitis • age at onset older than 40 years • cystic bone lesions • neurosarcoidosis • myocardial involvement • stage III or IV pulmonary disease
SARCOIDOSIS • Race • 10-17 times more common in African Americans than in whites • Whites present more commonly with earlier stage disease, usually bilateral hilar adenopathy • African Americans present at an earlier age with later stage disease • African Americans also have a greater likelihood of developing extrathoracic disease, lupus pernio, cystic bone lesions, chronic uveitis, chronic progressive disease, worse long-term prognosis, and a higher relapse rate • Lupus pernio also occurs with a higher frequency among Puerto Ricans than whites • Erythema nodosum more commonly effects the Scandinavian population • Cardiac involvement is more common in Japan than in other countries
SARCOIDOSIS • Sex • affects both men and women, but it seems to be most prevalent among African American women • The incidence is highest in African American women followed in order by African American men, white women, and white men. • Age • Although sarcoidosis can appear at any age, a bimodal age distribution is seen, which peaks between ages 25-35 and 45-65 years.
SARCOIDOSIS • Clinical • Because sarcoidosis can involve any organ system, the clinical presentation is often variable • Patients most commonly present in winter and early spring, which suggests a possible environmental trigger • The onset is usually insidious, and findings may be discovered on routine chest radiographs • Cutaneous involvement is seen in 25% of patients; it usually accompanies systemic involvement but may be the only site of involvement.
SARCOIDOSIS • General manifestations: One third of patients have constitutional symptoms, such as fever, fatigue, and weight loss. • Pulmonary system: The lungs are affected in most patients. Symptoms occur in one third to one half of patients and most commonly include dyspnea, dry cough, and chest tightness or pain. The disease can progress to parenchymal infiltration and, ultimately, irreversible fibrosis. • Lymphatic system: One third of patients have palpable lymph nodes that are moveable and nontender. Right paratracheal lymph node enlargement is most commonly seen, followed next by cervical nodes. • Ocular involvement: Anterior uveitis is the most common finding, which may be associated with fever and parotid swelling (also called uveoparotid fever). Chronic uveitis, most commonly occurring in African Americans, can lead to adhesions, glaucoma, cataract formation, and blindness. Although uveitis is most common, any part of the eye may be affected. • Neurosarcoidosis: Involvement of the nervous system occurs in fewer than 10% of patients; it may be lethal. The disease can affect any part of the nervous system. Seventh cranial nerve palsy is the most frequent finding. The pituitary gland and the hypothalamus may be involved. • Myocardial involvement: Clinically apparent cardiac involvement occurs in 5% of patients. • Other organs: Elevated liver function tests suggestive of hepatic dysfunction, arthritis, proximal muscle weakness, anemia, leukopenia, hypercalcemia, diabetes insipidus, and renal failure may be noted.
SARCOIDOSIS • Cutaneous involvement • is either specific or nonspecific • Histopathologically, specific lesions manifest as noncaseating granulomas, whereas nonspecific lesions do not reveal granulomas on histopathologic examination • Erythema nodosum is the main nonspecific cutaneous disease • lupus pernio, maculopapular, nodular, scar, plaque, angiolupoid, ichthyosiform, lichenoid, psoriasiform, and ulcerative lesions and subcutaneous nodules are examples of specific cutaneous disease
SARCOIDOSIS • EN is a hypersensitivity reaction resulting from exposure to a variety of infections or inflammatory disorders. • EN is usually an acute, self-limiting process and rarely requires treatment. Recurrences are uncommon. Tender, erythematous nodules are usually present on the extremities, most commonly on the anterior surface of the tibia. EN is more common in European, especially Scandinavian, women of childbearing age than in other people. • Löfgren syndrome is EN in conjunction with unilateral or bilateral hilar and/or right paratracheal lymphadenopathy, anterior uveitis, and/or polyarthritis. Other symptoms include fever, periarticular ankle inflammation, arthralgias, and pulmonary involvement. Löfgren syndrome is usually an acute disease with an excellent prognosis, typically resolving spontaneously in 6-8 weeks.
SARCOIDOSIS • Lupus pernio • characterized by red-to-purple or violaceous, indurated plaques and nodules that usually affect the nose, the cheeks, the ears, and the lips, but it can appear on the dorsa of the hands, the fingers, the toes, and the forehead. • usually more common in black women with long-standing systemic, usually pulmonary, sarcoidosis than in other people • also commonly seen with chronic uveitis and bone cysts • The course is usually chronic, and severe cosmetic disfigurement may result • Lupus pernio, especially involving the nasal rim, has been associated with granulomatous involvement of the upper respiratory tract (50%) and lungs (75%)
SARCOIDOSIS • Maculopapular sarcoidosis is the most common lesion seen in cutaneous sarcoidosis, especially in African American women • Granulomatous acne rosacea may mimic sarcoidosis clinically and histopathologically • Usually, lesions are asymptomatic, red-brown macules and papules commonly involving the face, the periorbital areas, the nasolabial folds, and/or the extensor surfaces. • Lesions usually resolve without scarring, although scarring may occur • These lesions may also occur in acute sarcoidosis.
SARCOIDOSIS • Plaque sarcoidosis is characterized by round-to-oval, red-brown to purple infiltrated plaques • the center of the plaque may be atrophic • Some plaques may even appear scaly and can be confused with lesions of psoriasis or lichen planus • most commonly occur on the extremities, the face, the scalp, the back, and the buttocks, and they may have an annular appearance • The distribution is usually symmetric • Angiolupoid sarcoidosis is a subtype that has a similar appearance but has large telangiectatic vessels in addition to the characteristics mentioned above • usually chronic; most patients have the disease for more than 2 years • can heal with scarring, and, if plaques involve the scalp, they may lead to alopecia • Patients with plaque lesions usually have more severe systemic involvement
SARCOIDOSIS • Subcutaneous nodular sarcoidosis • nontender, firm, oval, flesh-colored or violaceous nodules that are 0.5-2 cm in diameter. They are commonly found on the extremities or the trunk • usually appear in the beginning of the disease. These patients often have nonsevere systemic disease. • In some patients, the nodules resolve spontaneously.
SARCOIDOSIS • Infiltration of scars may occur • Scars from previous trauma, surgery, venipuncture, or tattoo may become infiltrated and show a red or purple color. • These lesions may be tender. • Sarcoidosis is called the "great imitator" because it can have almost any morphology • Other rare lesions of cutaneous sarcoidosis are • ichthyosiform • lichenoid, vasculitic • psoriasiform • erythrodermic • verrucous • papillomatous • ulcerative lesions
SARCOIDOSIS • Differential diagnosis: • Cutaneous tuberculosis • Lupus erythematosus • Drug erutions • Lymphocytoma cutis • Granuloma anulare • Necrobiosis Lipoidica • Granuloma Faciale • Psoriasis, • Ichthyosis • Syphilis • Leprosy • Tinea Corporis • Lichen Planus • Discoid Lupus Erythematosus
SARCOIDOSIS • Laboratory Studies • CBC count with differential and platelets • Leukopenia and/or thrombocytopenia are frequent findings. • Eosinophilia occurs in 24% of patients, and anemia occurs in 5% of patients. • Serum calcium and 24-hour urine calcium levels • Hypercalciuria has been found in 49% of patients in some studies, whereas 13% of patients had hypercalcemia. • Hypercalcemia occurs in sarcoidosis due to increased intestinal absorption of calcium that results from overproduction of a metabolite of vitamin D by pulmonary macrophages. • Serum angiotensin-converting enzyme (ACE) level • elevated in 60% of patients; therefore, this test is not sensitive in diagnosing sarcoidosis. • helpful in monitoring disease activity and treatment response. • ACE is derived from epithelioid cells of the granulomas, therefore, it reflects granuloma load in the patient. • Serum chemistries, such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, BUN, and creatinine levels: These levels may be elevated with hepatic and renal involvement. • Other: Elevated liver function tests suggestive of hepatic dysfunction, elevated erythrocyte sedimentation rate, elevated anti-nuclear antibodies (30%), diabetes insipidus, and renal failure may be noted.
Imaging Studies • Chest radiography • Radiographic involvement is seen in almost 90% of patients. Chest radiography is used in staging the disease. • Stage I disease shows bilateral hilar lymphadenopathy (BHL). Stage II disease shows BHL plus pulmonary infiltrates. • Stage III disease shows pulmonary infiltrates without BHL. • Stage IV disease shows pulmonary fibrosis. • CT of the thorax • Whole body gallium Ga 67 scanning
SARCOIDOSIS • Other Tests • Kveim test • This test is the most specific test for sarcoidosis. • It is not commonly available because of difficulty in obtaining a validated antigen source as well as a fear of transmitting infection. • The Kveim test involves intradermal injection of tissue from the spleen or the lymph node of a patient with sarcoidosis. A biopsy sample is obtained from the area 4-6 weeks after injection, and it is histologically examined for noncaseating granuloma formation, which, if found, indicates a positive result. • Tuberculin skin test • Patients with sarcoidosis have impaired delayed-type immune reactions. • Two thirds of patients have cutaneous anergy to the tuberculin skin test. • Pulmonary function test • The most common abnormalities found are defects in diffusing capacity and vital capacity. • Evidence of both restrictive abnormalities and obstructive abnormalities may be found. • Bronchoalveolar lavage with a CD4/CD8 ratio: A CD4/CD8 ratio of more than 3.5 has a specificity of 94% for sarcoidosis. • Electrocardiogram • to rule out unsuspected or asymptomatic arrhythmias or heart block. • Unsuspected ECG abnormalities may be seen in 10% or more of patients with systemic sarcoidosis, including Löfgren syndrome
SARCOIDOSIS • Biopsy of tissue • The skin is the most easily accessible tissue for biopsy. • Biopsy of all cutaneous lesions of sarcoidosis, except EN, is helpful because, histologically, EN is not specific for sarcoidosis. • Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis • Obtaining a biopsy specimen is extremely important in confirming the diagnosis of sarcoidosis. • Biopsy specimens need to be sent for histologic examination, and staining may need to be performed to rule out infectious causes of granuloma formation, including mycobacterial and deep fungal infections. • Tissue culture may be appropriate in some clinical settings, especially if fungal or atypical mycobacterial infections are suspected. • A biopsy sample of bronchial mucosa demonstrates the presence of noncaseating granulomas.
SARCOIDOSIS • Treatment • varies based on the symptoms and the organ systems involved in each patient. • Oral corticosteroids are usually the treatment of choice for patients with neurologic, cardiac, or ocular involvement not responding to topical corticosteroids; hypercalcemia; and symptomatic stage II and all stage III pulmonary disease. • Limited, nondisfiguring cutaneous involvement may be treated with topical or intralesional corticosteroids. • Infliximab is a promising option for those with recalcitrant or disfiguring disease. • Other agents that have been used to treat cutaneous sarcoidosis include cyclosporine, chlorambucil, oral isotretinoin, allopurinol, minocycline, doxycycline, psoralen with UVA, infliximab, etanercept, adalimumab, thalidomide, leflunomide, pentoxifylline, and melatonin, ACE inhibitor, photodynamic therapy with methyl aminolevulinate