Download
1 / 22
220 likes | 333 Vues
This document explores the California Pay-for-Performance (P4P) program's impact on healthcare quality and efficiency. Instituted under Executive Order 13410, the program aims to enhance care through four foundational goals: interoperability of health IT, transparency in quality measures and pricing, and promoting overall healthcare efficiency. Key findings showcase regional performance variations, modest improvements in clinical measures, and the influence of socio-economic factors on physician reimbursement, underscoring the need for balanced payment systems that encourage improvement without exacerbating disparities.

E N D
Tom Williams Executive Director Integrated Healthcare Association The Quality Colloquium Quality and Incentives: Value-Based Purchasing, Pay for Performance and Transparency August 20, 2008
National Leadership • HHS Secretary Leavitt inspired Executive Order 13410 • Four cornerstone goals - Interoperable Health IT - Transparency of Quality Measurements - Transparency of Pricing Information - Promoting Quality & Efficiency of Care • Ultimate Goal: “A Change in Culture”
IHA Sponsored California Pay for Performance (P4P) Program Health Plans: Aetna Blue Cross Blue Shield Western Health Advantage Medical Group and IPAs: 230 groups 35,000 physicians • CIGNA • Health Net of CA • Kaiser* • Pacificare/United 12 million HMO commercial enrollees * Kaiser participates in the public reporting only 4
California Pay for Performance: Summary of Performance Results Clinical: continued modest improvement on most measures 5.1 to 12.4 percentage point increases since inception of measure Patient experience: scores remain stable but show no improvement IT-Enabled Systemness: most IT measures are improving Almost two-thirds of physician groups demonstrated some IT capability Almost one-third of physician groups demonstrated robust care management processes Continued performance improvements but “breakthrough” point not achieved yet. 5
Lesson Wide variation across regions exists; contributes to overall “mediocre” statewide performance Big gains possible with focused attention on certain regions P4P Response Pay for and recognize improvement (20% of payment for 2007) More fundamental change in calculus of payment for improvement for 2008/09 California Pay for Performance: Regional Variability in Quality
Top Performing Groups MY 2006 Results by Region California Pay for Performance: Clinical Performance Variation
California Pay for Performance:A Tale of Two Regions Inland EmpireBay Area PCPs/100K Pop. 53 116 % Pop. Medi-Cal 17% 12% % Hispanic 43% 21% Per Capita Income $ 21,733 $ 39,048
California Pay for Performance:A Tale of Two Regions Clinical Performance P4P Performance Score
Are Quality Variations Correlated with Physician Reimbursement Disparities? The data and subjective experience suggest: Physicians in geographies with low socioeconomics receive disproportionately lower reimbursement across their practice, resulting in diminished physician and organizational capacity, reducing both access and quality of healthcare, even in a uniformly, well-insured population.
P4P Quality Payment Incentives • Fundamental reimbursement disparities appear to be the main culprit; however P4P should at a minimum not increase reimbursement disparities • Payment for absolute and relative performanceshould be balanced with payment for improvement
Paying for Improvement Survey Response: What % of total bonus payments by health plans should be allocated to improvement vs. relative performance? (n=200, IHA Stakeholders meeting, 10/4/07)
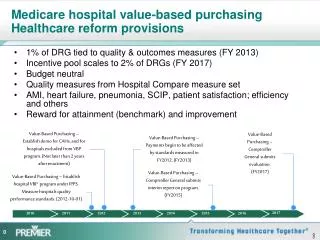
Paying for Performance & Improvement Excerpt from CMS Hospital Value-Based Purchasing Listening Session #2, April 12, 2007
Transparency – Public Reporting www.opa.ca.gov 14
Transparency – Public Reporting California General Public Survey, conducted by Harris Interactive (12/07)
Transparency – Quality Improvement Rates for Hip Revisions • Total hip revision rates (2006): • National average: 18% • Kaiser Permanente: 12.8% • Sweden: 7% Does this reflect more aggressive treatment, or less effective care? Slide attributed to Thomas Barber, MD, Permanente Medical Group, presented at the CAHP conference, October 2006.
Transparency – Quality Improvement Countries with National Joint Replacement Registries • 1975: Sweden- Knees • 1975: Sweden-Hips • 1980: Finland • 1987: Norway • 1995: Denmark • 1997: Germany • 1999: New Zealand, Australia • 2001: Canada, Romania • 2003: England, Wales, Slovakia • 2004: Switzerland
Transparency – Quality Improvement Why doesn’t the U.S. have mandatory device registries?
Cost and Quality Healthcare as Percentage of GDP • 60%+ of NME passes through public sector budgets (CMS, public employees, tax breaks, etc.) • Healthcare at 16.3% of GDP (2007) • Therefore, about 10% of GDP is healthcare spend passing through public sector budgets (.6 x 16.3% = 9.8%)
Cost and Quality Healthcare as Percentage of GDP • Total tax revenues in U.S. (federal, state, local) equals about 28% of GDP • So, healthcare uses about 1/3 of public sector budgets (.098/28% = 35%) and growing! • Healthcare at 20% of GDP = 43% of public sector budgets
Cost and Quality Example: Michigan “Checklist”: • Over 18 months, reduced infections in ICU by 66% • Estimated 1,500 lives saved • Estimated $100 million saved
California Pay for Performance For more information: www.iha.org (510) 208-1740 Pay for Performance has been supported by major grants from the California Health Care Foundation