Drug-Herb Interaction
Drug-Herb Interaction. Presented by: Dr.Rania Magadmi. . . The aim of this presentation is to highlight the clinicalinteractions between herbal product and prescribeddrugs. Outlines:. Mechanism of Drug- Herb interactions Literature review Systematic review


Drug-Herb Interaction
E N D
Presentation Transcript
Drug-Herb Interaction Presented by: Dr.Rania Magadmi
. The aim of this presentation is to highlight the clinicalinteractions between herbal product and prescribeddrugs
Outlines: • Mechanism of Drug- Herb interactions • Literature review • Systematic review • Strategies to minimize Drug-Herb interaction
Introduction Outlines: • Surveys show that two-thirds of womenuse herbs for perimenopausal symptoms, 45% of parentsgive their children herbal treatments and 45% ofpregnant women try herbal remedies. • 16% of prescription drug users consume herbal sup-plements
Mechanism of Interaction: • The altered drug response of herb-drug interactions depends on factors related to:
Pharmacokinetic Pharmacodynamic
Cytochrome P450 • Many herbs (e.g. St John’s wort, kava and garlic,. coumarins and caffeine) have been identified as substrates, inhibitors and/or inducers of CYP enzymes. CYP CYP
P-glycoprotein • Like CYP, P-glycoprotein could cause inhibition, activation, or induction by herbs. Curcumin, ginsenosides, piperine, sylimarin and catechins may affect P-glycoprotein-mediated drug transport. St John’s wort induces the intestinal expression of P-glycoprotein both in isolated cells and in healthy volunteers.
Pharmacodynamic • A few pharmacodynamic interactions have also been described. Pharmacodynamicinteractions may be synergetic(e.g. interaction between the anticoagulant warfarinwith antiplatelet herbs), or antagonistic (e.g. kava possesses dopaminergic antagonistic propertiesand hence might reduce the pharmacological activity ofthe anti-parkinson drug levodopa) .
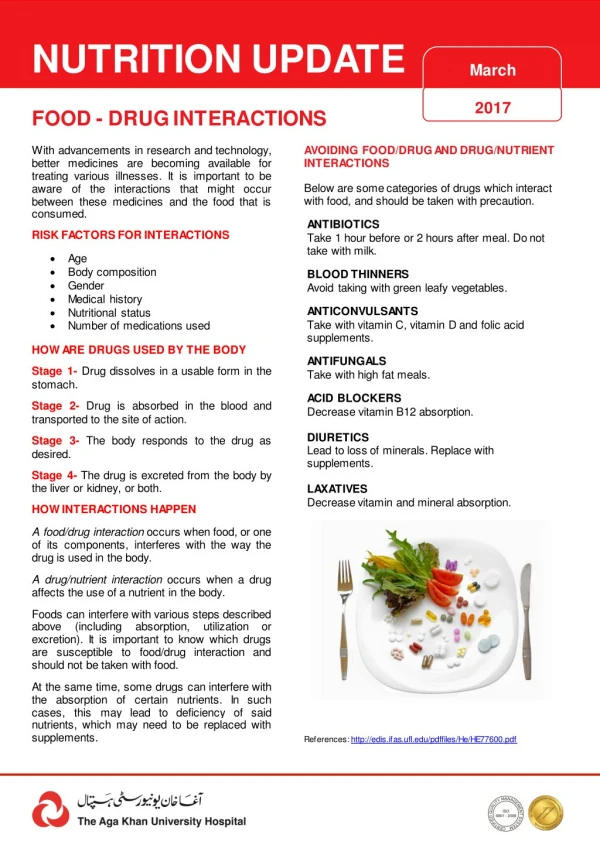
Literature Review: • The World Health Organization (WHO) defines herbal supplements as "Finished, labelled, medicinal products that contain active ingredients from aerial or underground parts of plants, or other plant material, or combinations of, whether crude state or as other preparations “. WHO Programm on Traditional Medicines: Guidelines for the assessment of herbal medicines. Geneva: World Health Orginization, 1991.
Literature Review: • 32 drugs interacting with herbal medicines in humans. • E.g. anticoagulants (warfarin, aspirin and phenprocoumon) • sedatives and antidepressants (midazolam, alprazolam&amitriptyline) • oral contraceptives • anti-HIV agents (indinavir, ritonavir and saquinavir) • cardiovascular drug (digoxin) • immunosuppressants (cyclosporine and tacrolimus) • anticancer drugs (imatinib and irinotecan).
Evidence for herb-drug interactions • Case reports • Unreported? 70% “don’t ask-don’t tell” • Lab studies • Define mechanisms • Recent interest in CYP450 induction • Human studies • Trials using probe drugs • May be done on healthy population • Genetic polymorphisms De Smet, Br J Clin Pharm 2006; 63:258-67
Drugs that have been reported to interact w herbs Current Pharmaceutical Design, 2006,Vol. 12, No. 35
Drugs that have been reported to interact w herbs Current Pharmaceutical Design, 2006,Vol. 12, No. 35
Drugs that have been reported to interact w herbs Current Pharmaceutical Design, 2006,Vol. 12, No. 35
Drugs that have been reported to interact w herbs Current Pharmaceutical Design, 2006,Vol. 12, No. 35
Interactions with CVS Pharmacotherapy: • The majority of reports concern drugs with a narrowtherapeutic index such as warfarin and digoxin. • Increasedanticoagulant effects could be expected when warfarinis combined with coumarin-containing herbs (e.g.boldo, fenugreek, papaya , mango) or with antiplatelet herbs(e.g. danshen, garlic, ginkgo). • Vitamin K containing herbs (e.g. green tea) can antagonized the anticoagulant effect of warfarin.
Grant P. Warfarin and cranberry juice: an interaction.J. Heart. Valve Dis. (2004) 13 25–26. Six weeks after starting cranberry juice a 70-year-old man under warfarin was admitted to hospital with an INR >50. He died of a gastrointestinal and pericardial haemorrhage. (Cranberry juice contains antioxidants, including flavonoids, which are know to inhibit CYP enzymes)
Interactions with cardiac inotropic drugs In a single-blind, placebo-controlled study . clinical trials
Interactions with antihypertensive drugs • Surprisingly, an elderly patient was found to have anincrease in blood pressure after taking ginkgo (a peripheral vasodilator) while receiving a thiazide diuretic. • There is no rationalpharmacological mechanism to explain this unusualinteraction.
Interaction with oral hypoglycemic drugs • Clinical studies have shown that gumguar reduced the absorption of metformin andglibenclamide. By contrast, anothertrial showed that gum guar enhanced the insulinogenicand blood glucose lowering effect of glibenclamide. • A fall in glucose levels has been reported in a 40-year-old diabetic woman taking chlorpropamide and garlic. This event is likelybecause of an additive effect on glucose level . Capasso F., Gaginella T.S., Grandolini G., Izzo A.A. Phytotherapy. A quick reference to herbal medicine, SpringerVerlag, Berlin, Heidelberg, 2003.
INTERACTIONS WITH ANTI-INFLAMMATORY DRUGS • Many paper showed that Liquorices increased the plasma prednisolone concentrations in six healthy men. • Glycyrrhizin, which is astrong inhibitor of 11 beta-hydroxysteroiddehydrogenase ,influences prednisolone pharmacokinetics by inhibiting its metabolism. Chen M.F., Shimada F., Kato H., Yano S., Kanaoka M. Effect of oral administration of glycyrrhizin on the pharmacokinetics of prednisolone. Endocrinol. Jpn. (1991) 38 167–174.
STRATEGY FOR ELIMINATING TOXICITYARISING FROM DRUG-HERB INTERACTIONS 1. PredictingDrug-Herb Interactions • It is necessary to assess the clinical risks by predicting qualitatively and quantitatively drug-herb interactions.
STRATEGY FOR ELIMINATING TOXICITYARISING FROM DRUG-HERB INTERACTIONS 2. Identification of Drugs that Interact with Herb • The identification of drugs causing drug-herb interactions and the mechanisms involved are important in term of rational use of therapeutic drugs. • The application of high throughput approaches to the study of drug-herb, herb-CYP and herb- PgP interactions is becoming possible. If potential toxic drug-herb interactions have been observed, the combined use of related drugs and herbs should be generally avoided. In some cases where the avoidance is difficult, proper dose adjustment or alternative drugs may be needed.
STRATEGY FOR ELIMINATING TOXICITYARISING FROM DRUG-HERB INTERACTIONS 3. Therapeutic Drug Monitorin Due to frequent pharmacokinetic drug-herb interactions, monitoring of plasma concentrations of drugs with narrow therapeutic indices are always important in patients also taking herbs.
STRATEGY FOR ELIMINATING TOXICITYARISING FROM DRUG-HERB INTERACTIONS 4. Design of Hard Drugs to Eliminate Toxicity Arising from Drug-Herb Combinations • It appears that the chemical properties of a drug critical for herbal interaction include (i) being a CYP substrate, (ii) being a PgP substrate, (iii) Induction/ inhibition of CYP
Hard drugs :not metabolized by CYPs and/or not transported by PgP. • Example: bisphosphonates (e.g. etidronate and alendronate,) and certain ACE inhibitors (e.g. enalaprilat and lisinopril).
Conclusion • Although some drug– herb interactions may be clinically insignificant (e.g. interaction between gum guar andpenicillin V), others may have serious consequences (e.g.interaction between St John’s wort and cyclosporine). • Withdrawal of a chronically administered herbal product that acts as an inducer in a patient stabilized on effective drug therapy can result in untoward pharmacological or toxic effects
limitation • Reported drug-herb interactions are ANECDOTAL (single reports). • Herbal medicines are mixtures of more than one active ingredient. makes it difficult to draw useful comparisons between clinical studies or case reports. • The likelihood of herb±drug interactions could be higher than drug±druginteractions. • fewer than 40% of patients disclose their herbal supplement usage to their physician and many physicians are unaware of the potential for– drug herb interactions .
Checking for herb-drug interactions • Natural Standard (www.naturalstandard.com). Subscriptions for PDA/desktop available. • Partial database at MedlinePlus.gov • Natural Medicines Comprehensive Database (www.naturaldatabase.com). Subscription service.
Induction • Induction is a term used to describe a physiologica adaptive response to continued xenobiotic exposure. It is characterized by enhanced gene transcription and/ortranslation, stabilized messenger ribonucleic acid, or inhibited protein turnover. The end result can be increased amounts of proteins that determine drug disposition such as metabolic enzymes or transporters. The dose of the inducer determines its cellular concentration and hence the extent of induction. The resulting clinical effects usually start within a few days of repeated administration. After withdrawal of the inducer, reversal is generally complete within 1 week. • Case reports of reduced exposure and reduced degree and/or duration of drug response have often served as mportant stimuli for formal study of herbal–drug interactions [10]. A common in vivo method uses a drug probe that is a relatively safe substance inactivated or eliminated primarily by a single metabolic process (e.g. midazolam and cytochrome P450(CYP)3A4) or transport process (e.g. fexofenadine and P-glycoprotein). increasingly popular is the use of probe ‘cocktails’ that determine the activities of multiple eliminating pathways on a single occasion. The probes are administered before and then after a suitable treatment period with a particular herbal product to examine their effects on clearance of the probe. • The molecular mechanisms that govern the inductive response are well established and in vitro tools are available to predict whether herbal products or their chemical constituents might cause a clinically important drug interaction. The most prominent mechanisms for induction are ligand-dependent transcriptional activation of nuclear receptors, such as the pregnane X (PXR), constitutive androstane (CAR) or aryl hydrocarbon receptors (AhR). Convenient cell-based screening assays for activation of nuclear receptors are routinely used. Further investigations in the cultured primary human hepatocyte model are performed to confirm induction of gene expression.