Download
1 / 25
250 likes | 394 Vues
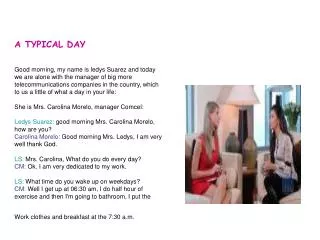
In this case study from a TB clinic, we explore the management of four patients, each with a positive PPD test but normal chest X-rays. A 35-year-old man seeks hospital employment, a 64-year-old woman is referred for immigration, and an 18-year-old young woman also has immigration purposes. Additionally, a 54-year-old man, previously an IV drug user, shows a more significant risk factor. We will discuss their potential TB disease risk, the application of IGRA testing, and whether they should receive treatment for latent TB infection (LTBI).

E N D
A typical day in the TB clinic You see the following patients in the TB clinic. All have normal CXRs: • A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam. He wants to work in your hospital. • A 64 year old woman from Jamaica with a 12 mm PPD who is referred for immigration purposes. She has no risk factors and her exam is negative • An 18 year old young woman from Lima, Peru with a 14 mm PPD for immigration purposes. Her history and exam are negative • A 54 year old man born and raised in Hartford, who has a 20 mm PPD. He cannot recall having had a previous TST. He used to be an IV drug abuser. He says his HIV was negative 3 months earlier. What is the risk of developing TB disease and what is the role, if any, for IGRA testing in these patients, and how would you treat them?
Interpretation of TST Results nyc.gov/health
False-positive and false-negative PPDsThe PPD is only about 70% sensitive • False positive • BCG vaccination • Nontuberculous mycobacterial infection • Improper administration or interpretation • False negative • Very young (<6 months old) • Inability to mount an immune response (e.g., HIV or TB itself) • Recent infection (<10 weeks since exposure) • Very remote infection • Recent live virus vaccination • Improper administration or interpretation
Interferon Gamma Release Assays (IGRAs) Quantiferon Gold/Gold In-Tube (QFT-GIT) 2nd/3rd generation tests Available from commercial labs ELISA that measures amount of IFN-gamma released by patient’s cells T-Spot.TB Approved July 2008 Elispot
Indeterminate IGRA • Less frequent with QFT-GIT • Several possible reasons • High background IFN-: patient illness, mitogen in wrong well, defective tubes • Low mitogen: immune suppression, defective tubes, overfilling, inadequate shaking • Options? • Repeat QFT • Place TST instead
Comparison of IGRAs and TST IGRA • About 70% sensitive • Not affected by BCG • Not cheap • New: less experience • In vitro testl; requires phlebotomy • No boosting • Only need 1 patient visit • Gives numbers, lessens variability • Results possible in 1 day • May decline in response to test after treatment TST • About 70% sensitive • Fairly specific • Cheap • Been around a long time • In vivo test • Potential boosting • Requires 2 patient visits • Inter-reader variability • Results in 2-3 days • May be more sensitive in detecting remote infections
Potential to cause big problems versus the hassle required to reduce this risk
Latent Tuberculosis Infection (LTBI) and progression to real disease About 5–10% of persons with LTBI will develop TB disease if untreated 50% in the first two years 50% later in life The most effective treatment would be to identify and treat LTBI in all these individuals However, treatment of LTBI is: Is lengthy: 4 to 9 months, generally Is costly: not from medications but because patients have to come in regularly for monitoring, thereby missing work, school, etc. Carries a very small but real risk for side effects
High Risk for Conversion of LTBI to TB Disease Recent infection, documented conversion (within the last 2 years) HIV infection Substance abuse (alcohol or drugs) Old healed TB lesions on CXR Children under 5 years of age Certain medical conditions
Medical Conditions HIV infection <90% of ideal body weight, recent weight loss Diabetes mellitus (poorly controlled) Chronic renal failure Solid organ transplant recipients Certain cancers and / or treatment Higher-dose steroid treatment (15mg, >4 weeks) Tumor necrotizing factor antagonist therapy (TNF-α antagonists) History of gastrectomy or jejunoileal bypass surgery
The Online TST/IGRA Interpreter: https://www.tstin3d.com
Statistics and risks derived from website (1) A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam, normal chest x-ray. He wants to work in your hospital. What do you think? Should he be offered LTBI rx? Stats from history as given above: Likelihood of a true positive PPD: 100% Annual risk of TB disease: 0.1% Lifetime risk of TB disease: 4.5% Risk of hepatotoxicity from treatment: 0.2%
Statistics and risks derived from website (2) A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam, normal chest x-ray. He wants to work in your hospital. New data: the patient had diabetes: What do you think? Should he be offered LTBI rx? Likelihood of a true positive PPD: 100% Annual risk of TB disease: 0.28% (originally 0.1%) Lifetime risk of TB disease: 12.6% (originally 4.5%) Risk of hepatotoxicity from treatment: 1.2%
Statistics and risks derived from website (3) A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam, normal chest x-ray. He wants to work in your hospital. New data: the patient had documented close contact: What do you think? Should he be offered LTBI rx? Likelihood of a true positive PPD: 100% Annual risk of TB disease: 0.10% Lifetime risk of TB disease: 9.3% (originally 4.5%) Risk of hepatotoxicity from treatment: 1.2% Risk of developing TB in next two years: 5% (originally 1.2%)
Statistics and risks derived from website (4) A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam, normal chest x-ray. He wants to work in your hospital. New data: patient had documented new infection (< 2 years): What do you think? Should he be offered LTBI rx? Likelihood of a true positive PPD: 100% Annual risk of TB disease: 0.10% Lifetime risk of TB disease: 5.8% (originally 4.5%) Risk of hepatotoxicity from treatment: 1.2% Risk of developing TB in next two years: 1.5% (originally 1.2%)
Statistics and risks derived from website (5) A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam, normal chest x-ray. He wants to work in your hospital. New data: the patient had a granuloma on chest x-ray What do you think? Should he be offered LTBI rx? Likelihood of a true positive PPD: 100% Annual risk of TB disease: 0.2% (originally 0.10%) Lifetime risk of TB disease: 9% (originally 4.5%) Risk of hepatotoxicity from treatment: 1.2% Risk of developing TB in next two years: 1.5% (originally 1.2%)
Statistics and risks derived from website (6) A 35 year old man from Hartford with a 16 mm positive PPD. He has no known exposure to MTB, no risk factors, normal exam, normal chest x-ray. He wants to work in your hospital. New data: Abnormality (more than a granuloma) on chest x-ray: What do you think? Should he be offered LTBI rx? Likelihood of a true positive PPD: 100% Annual risk of TB disease: 1.25% (originally 0.10%) Lifetime risk of TB disease: 56% (originally 4.5%) Risk of hepatotoxicity from treatment: 1.2%
Statistics and risks derived from website (7) A 64 year old woman from Jamaica with a 12 mm PPD who is referred for immigration purposes. She has no risk factors and her exam is negative. She came to USA 10 years ago. What do you think? Should she be offered LTBI rx? Stats: Likelihood of a true positive PPD: 62% Annual risk of TB disease: 0.06% Lifetime risk of TB disease: 0.99% Risk of hepatotoxicity from treatment: 2.3%
Statistics and risks derived from website (8) A 64 year old woman from Jamaica with a 12 mm PPD who is referred for immigration purposes. She has no risk factors and her exam is negative. She came to USA 10 years ago. New data: she is taking a TNF alpha drug: What do you think? Should she be offered LTBI rx? Likelihood of a true positive PPD: 62% Annual risk of TB disease: 0.33% (originally 0.06%) Lifetime risk of TB disease: 5.3% (originally 0.99%) Risk of hepatotoxicity from treatment: 2.3%
Statistics and risks derived from website (9) A 18 year old from Lima, Peru with a 14 mm PPD for immigration purposes. She has been in USA for 2 years. Her history and exam are negative What do you think? Should she be offered LTBI rx? Stats: Likelihood of a true positive PPD: 91% Annual risk of TB disease: 0.07% Lifetime risk of TB disease: 5.6% Risk of hepatotoxicity from treatment: 0%
Statistics and risks derived from website (10) A 54 year old man born and raised in Hartford, who has a 20 mm PPD. He cannot recall having had a previous TST. He used to be an IV drug abuser. He says his HIV was negative 3 months earlier. What do you think? Should he be offered LTBI rx? Stats: Likelihood of a true positive PPD: 100% Annual risk of TB disease: 0.25% Lifetime risk of TB disease: 6.5% Risk of hepatotoxicity from treatment: 2.3%
Statistics and risks derived from website (11) A 54 year old man born and raised in Hartford, who has a 20 mm PPD. He cannot recall having had a previous TST. He used to be an IV drug abuser. He says his HIV was negative 3 months earlier. New data: the patient is HIV positive What do you think? Should he be offered LTBI rx? Likelihood of a true positive PPD: 100% Annual risk of TB disease: 8% (originally 0.25%) Lifetime risk of TB disease: 100% (originally 6.5%) Risk of hepatotoxicity from treatment: 2.3%





![A Typical Day in the Life of a Translator [Infographic]](https://cdn4.slideserve.com/9739188/slide1-dt.jpg)