Download
1 / 70
740 likes | 2.48k Vues
Review of START and JumpStart Triage. Condell Medical Center EMS System ECRN Disaster Training Module March 2009 Material development by Illinois EMSC and children’s Memorial Hospital. Modified for CMC staff by Sharon Hopkins, RN, BSN, EMT-P. Rationale for the Packet.

E N D
Review of START and JumpStart Triage Condell Medical Center EMS System ECRN Disaster Training Module March 2009 Material development by Illinois EMSC and children’s Memorial Hospital. Modified for CMC staff by Sharon Hopkins, RN, BSN, EMT-P
Rationale for the Packet • Without training you will be ill-prepared to respond to a disaster/multiple patient incident • START and JumpSTART triage is the triage process in the Region X Multiple Patient Plan for disaster management • This training is to review the triage processes referred to as START for the adult and JumpStart for the pediatric patient • This triage is usually performed in the field but can be adapted to be performed in the ED
Pediatric Disaster TriageUtilizing the JumpSTART MethodMarch 2009 Development of this educational program was sponsored by Illinois EMSC and Children’s Memorial Hospital and supported in part by an Assistant Secretary for Preparedness and Response (ASPR) grant. This program was adapted from a module developed through HRSA funding by the Chicago Department of Public Health. Program adapted to Condell ECRN CE by Sharon Hopkins, RN, BSN 3.09
Disclaimer NOTE: This slide set and all related training information provided in this session is in accordance with current practice at the time that this program was developed. This program was developed utilizing federal grant funding, therefore all training materials are considered under public domain and can be utilized by others in the conduction of similar educational programs, provided there is acknowledgement of the source of these materials. When using these training materials, please include appropriate acknowledgements which can be found on the last slide in this presentation. These training materials are available on the Illinois EMSC website http://www.luhs.org/emsc
Objectives • Review unique pediatric issues in a disaster situation • Review incorporating pediatrics into your disaster planning • Review triage and the pediatric patient • Review START and JumpSTART triage • Complete triage scenario exercises in the packet • Complete the quiz with a score of 80% or better
Disaster “A medical disaster occurs when the destructive effects of natural or man made forces overwhelm the ability of a given area or community to meet the demand for health care.” ACEP Policy Statement June 2000
Mass Casualty Incident Any incident in which there are more patients than rescuers with inadequate resources to immediately care for them
Natural Disasters At least 19 dead, including 8 at the high school as tornadoes rip through the South. • Earthquake • Flood • Snow/ice storm • Tornadoes • Others March 2, 2007 Enterprise, Alabama
Terrorist events • Arson • Bombings • Shootings • Use of chemical, biological or nuclear agents
The Old Way of Thinking… Kids were secondary victims of terrorism and inadvertently targeted
The new way of thinking … Children may be intentionally targeted Photo courtesy of Charles H Porter IV
Illinois Demographics • Illinois is the 5th most populous state with a population of 12.7 million • Over 3 million children <18 years of age • 900,000 are age five and younger. • Percent of Illinois children <18 y/o increased 10% between 1990 - 2000 • In the event of a disaster or terrorist event, children would be one of our most vulnerable populations
Basic Pediatric Differences Airway • Mouth and nose are smaller • More easily obstructed • Infants are nose breathers so secretions can be a major issue • Trachea is much shorter • ETT can be displaced easier • Narrow Airways • Easily obstructed • Diaphragm • Infants depend on diaphragm to breathe so abdominal distention can be problematic Oral explorers • Germs with feet
Large Head = Risk of headinjury Large unprotected intraabdominal organs = Risk liver, spleen & bowel injury Large Body Surface area = hypothermia
Vulnerability of Children: Anatomic & Physiologic Issues • Children are particularly vulnerable to aerosolized biological or chemical agents and radiation • Some agents (e.g., Sarin and Chlorine and radiation) are heavier than air and accumulate close to the ground—in breathing zone of children. • Children have faster ventilatory rates than adults • Inhale larger doses of the substance in the same period of time.
Vulnerability of Children: Anatomic & Physiologic Issues • Thinner skin and proportionately greater Body Surface Area (BSA) • Increased risk for hypothermia during field decontamination and treatment • Increased susceptibility to chemical agents • Vesicating agents (Nitrogen/Sulfur Mustard, Lewisite) • Nerve agents (Sarin, VX, Tabun, Soman) • Irritants and corrosives (chlorine, ammonia, phosgene) • Increased susceptibility to infections • Newborns • Children with chronic illnesses
Vulnerability of Children: Anatomic & Physiologic Issues A child’s condition can rapidly go from stable to life-threatening • Children have smaller circulating blood volumes than adults. • They have less blood and fluid reserves • More vulnerable to the effects of agents that produce vomiting and/or diarrhea -- can become dehydrated faster • Blood/fluid loss can lead to irreversible shock or death • More sensitive to changes in body temperature • Higher basal metabolic and cellular growth rates • Increased susceptibility to radiation, chemical agents • Increased leukemia and cancer risk to radiation exposed children age < 5y/o
Vulnerability of Children : Developmental Considerations • Can’t anticipate, recognize or flee from dangerous situations • Fear of strangers – inability to cooperate or communicate with officials/providers • Family separation – unaccompanied minors • Sensitive to emotional state of parents • Children, Terrorism & Disasters Toolkit (AAP) at www.aap.org further identifies these vulnerabilities
Decon Considerations • Unlikely to be cooperative • Will be frightened of process and staff in protective gear • Hypothermia risk • Slippery when wet • How best to get them through the decon shower system • Laundry baskets • Car seats with padding removed. Strap them in. • Hospital plastic bassinettes • Stretcher or conveyor system • Strip them, including the diaper!
“Hello. Come with me. I’m going to take you thru this shower over here”
Decon Considerations • Warm Water • High Volume/Low Pressure • Keeping the family unit together as much as possible • How will they hear you? • Showering process will take more time with children • Identification issues
Lessons learned • Decontamination of kids is “not a fun time” • Decon brushes can be rough on skin • Blankets, booties and towels work well • Age specific decision tree • Use ink markers to write directly on skin to identify
EMS systems need plans to establish communication and restore unity of families
Kids come with Parents You can find the CHAD sticker order form at www.dot.il.gov Using the tool bar; select Doing Business From the drop-down menu select Forms Click on Traffic Safety Forms Scroll down to the bottom Select TS 2268 Public Information and Education Materials Fax your completed form to (217) 557-5937 or mail it to Melissa Schaive, Illinois Department of Transportation 3215 Executive Park Drive, Springfield, IL 62794 Pediatric Identification
School Identification Pediatric Identification Medical History School identification
Children with Special Health Care needs (CSHCN) • Technology Dependent • Ventilators • G-Tubes • Shunts • Insulin Pumps • Developmentally Disabled • Chronic Diseases • Immunocompromised • Psychiatric/Behavioral Illnesses
Children with Special Health Care needs (CSHCN) • 18% (13.5 million) of U.S. kids meet criteria • Over 20,000 families in Illinois receive services from the Division of Specialized Care for Children (DSCC) • CSHCN are disproportionately poor & socially disadvantaged • Strong need for healthcare provider education & awareness
Key Principles of Medical Care Conventional Medical Care The objective of conventional medical care is to… Do the greatest good for the individual patient. Disaster Medical Care The key principle of disaster medical care is to… Do the greatest good for the greatest number of patients. Briggs, S and Brinsfield, K (eds), Advanced Disaster Medical Response for Providers. Harvard Medical International, 2003.
Triage • “To Sort” • Look at medical needs and urgency of each individual patient • Triage in Daily Emergencies • Do the best for each individual • Disaster Triage • Do the greatest good for the greatest number • Make an impossible task manageable
Triage • Primary Triage • Triage that is performed at the scene or point of first contact with patients. • Secondary Triage • Triage that is performed after further intervention is provided. Usually done in a medical sector.
80% of casualties self or buddy transport to the closest hospital
Important Triage Concepts • Helps to prioritize patients in a systematic and organized fashion • Helps in resource allocation • Provides an objective framework for stressful and emotional decisions • MCI (mass casualty incident) triage is different than daily triage, in both field and ED settings
MCI (Mass Casualty Incident) Triage • In order for MCI triage to work effectively, all victims must have equal importance at the time of primary triage. • No patient group can receive special consideration other than that dictated by their physiologic state. This includes children! Adapted from the Dr. Lou Romig slide set available at www.jumpstarttriage.com/
Triage Categories • RED - Immediate/emergent • YELLOW - Urgent • GREEN - Nonurgent • BLACK- Dead/little to no hope of survival BLACK RED YELLOW GREEN
RED - Immediate • Severely injured but treatable injuries and able to be saved with relatively quick treatment and transport • Examples • Severe bleeding • Shock • Open chest or abdominal wounds • Emotionally out of control
Yellow - Delayed Injured and unable to walk on their own. Potentially serious injuries but stable enough to wait a short while for medical treatment • Examples • Burns with no respiratory distress • Spinal injuries • Moderate blood loss • Conscious with head injuries
Green – Non-Urgent • Minor injuries that can wait for a longer period of time for treatment. • May or may not be able to ambulate • Examples • Minor fractures • Minor bleeding • Minor lacerations
Black - Deceased • Dead or obviously dying. May have signs of life but injuries are incompatible with survival. • Handle based on local protocols • Examples • Cardiac arrest • Respiratory arrest with a pulse • Massive head injury • Can be psychologically difficult to tag a child as black
Review of START and JumpSTART MCI Triage Tools Photo courtesy of Miami Dade Fire Rescue © Lou Romig MD, 2006. Used with permission.
START • Simple Triage and Rapid Transport • Joint development by the Fire & Marine Department and Hoag Hospital in New Port Beach, California • Gold standard for field adult MCI triage in U.S. and numerous other countries • Utilizes the standard four color triage categories • Used for primary triage • More information at www.start-triage.com
START vs JumpSTART Triage • START triage • Used for the adult population (non-pediatric) • JumpSTART • Used when the victim appears to be a child • Adult and pediatric patients do not share the same normal values for vital signs hence the need for 2 different tools • At approximately age 8, the pediatric patient is similar anatomically with the adult airway
ED Triage • Primary START or JumpSTART triage does not have to be repeated at the point of entry to the ED when patients are transported by EMS • But, not all patients will come by EMS • Historically, we know patients will self-transport • Triage will be a valuable tool to perform quick sorting when dealing with multiple patients at one time
Understanding Field Triage • The ED staff need to understand the triage performed in the field • Helps with the flow of continuity of care • If ED staff understand START and JumpSTART triage, they will understand how EMS made the decisions they did • START and JumpSTART triage is a process that can be duplicated and performed in the ED as needed – not all patients come by EMS!!!
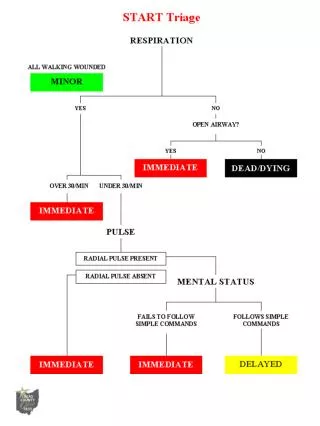
START Triage • This is just the 1st process of triage • It is meant to quickly and initially separate those with life threatening injuries from the less seriously wounded/ill • Secondary triage will allow retriage of a patient • Patient may be placed into a different triage category • Decision will be based on physiological criteria • START triage attempts to remove the emotional reaction from the decision process
START Triage • Start at the top of the algorithm • As soon as patient has been categorized, stop assessment and move onto the next patient • Triage proceeds through a process • Can patient get up and walk to triage area? • Evaluate respirations (presence & rate) • Evaluate circulation (capillary refill) • Evaluate neurological status (obeys simple commands)
JumpSTART Triage • Pediatric patients do not fit the START triage criteria • The youngest of our patients don’t walk yet • Respiratory rates are different • Circulation assessment is altered • Ability to follow directions changes with age • START triage has been modified to be able to be applied to this unique population