Cardiorespiratory Testing
Cardiorespiratory Testing. Maximal Oxygen Uptake. . AKA VO 2 Max Criterion measure of cardiorespiratory fitness Product of maximal cardiac output and arterial-venous oxygen difference Directly related to functional capacity of the heart. Maximal Oxygen Uptake. Direct measurement

Cardiorespiratory Testing
E N D
Presentation Transcript
Maximal Oxygen Uptake . • AKA VO2 Max • Criterion measure of cardiorespiratory fitness • Product of maximal cardiac output and arterial-venous oxygen difference • Directly related to functional capacity of the heart
Maximal Oxygen Uptake • Direct measurement • Open-circuit spirometry • Pulmonary ventilation • Expired O2 and CO2 fractions
Maximal Oxygen Uptake • Indirect methods • Estimation techniques • VO2 values correlated with intensities reached • Similarities in fitness levels • Similarities in age and gender • Regression equations used to predict VO2 . .
Maximal Oxygen Uptake • Indirect methods • Estimation techniques • Step tests • Little equipment or skill needed • Short duration test – less than 5 minutes • Requires some balance • Difficult for extremely deconditioned
Maximal Oxygen Uptake • Indirect methods • Estimation techniques • Field tests – practical (mass testing) • Cooper 12 minute run • Requires maximal effort & motivation • Unmonitored – danger for at-risk? • Rockport 1 mile walk • Requires maximal effort & motivation • Unmonitored but walking vs. running decreases danger
Maximal Oxygen Uptake • Indirect methods • Estimation techniques • Treadmill tests • Accommodates all fitness levels – speed changes • Requires skill and balance for some – practice? • Difficult to measure BP
Maximal Oxygen Uptake • Indirect methods • Estimation techniques • Cycle ergometer tests • Easy to take BP measurements • Non weight bearing – accommodates extremely weak • Small work rate adjustments can be made • Familiar skill – but not a common activity • Severe localized fatigue - motivation • Specific pedal cadence is required - motivation
Maximal Oxygen Uptake • Maximal Exercise Tests • Advantage • True maximal capacity can be measured • Increased sensitivity in Dx of CAD in asymptomatic • Disadvantage • Volitional fatigue • do they know maximum? • risk of injury • Physician supervision* • Emergency equipment*
Maximal Oxygen Uptake • Maximal Exercise Tests • Incremental workloads • Steady state not required • “Quick and dirty” • Just max is the goal • Prolonged – other measures along the way • Ventilatory threshold • Lactate threshold
Maximal Oxygen Uptake • Submaximal Exercise Tests • Assumptions • Steady is state reached at each work rate • Linear relationship between HR and work rate • Maximal HR is uniform for every age • Predict max from slope of line
Submaximal Testing • Keys to success • 2-3 min warm-up and equipment acquaintance • Monitor HR & BP near the end of each stage • Perceived exertion (6-20 or 1-10 scale) • Monitor subject’s/client’s appearance • Terminate at 85% of age-predicted max HR, or 70% of HR reserve, or if problems arise • Allow warm-down & monitor
Submaximal Testing • Test Termination Criteria in Low-risk adults (Box 4-5) • ***Subject requests to stop*** • **Failure of testing equipment** • Onset of angina – pain associated with ischemia • Significant rise or drop in BP • Signs of poor perfusion – pallor • Failure of HR to increase with workload increase • Noticeable change in heart rhythm • Severe fatigue
Submaximal Testing • Cycle Ergometer Tests • Astrand-Rhyming Cycle Ergometer Test (page 70) • Single stage test – target HR from 125-170 • Work Rate – (@ 50 rpm) • Men – unfit 300 or 600, fit 600 or 900 kgm/min • Women – unfit 300 or 450, fit 450 or 600 kgm/min • Heart rate taken @ 5th & 6th min. – average them • Use of nomogram to estimate max VO2 (Figure 4-1) • Correct VO2 max by multiplying correction factor for age difference in max HR . .
Submaximal Testing • Cycle Ergometer Tests • YMCA Cycle Ergometry Test (page 74) • 2 - 4 stage continuous exercise • Branching – if ___ Hr, then ___ intensity • Heart rate taken @ 2nd & 3rd min. of each stage • HR must be within 6 beats to go to next stage • HR must be between 110 and 85% age predicted max • Plot HRs of last min. then extrapolate to max HR • Line to predicted work rate at max VO2 • Calculate a predicted VO2 (Appendix D) . .
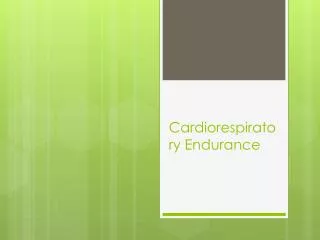
Max HR 220-age Submax 2 Submax 1 Max Work Rate Work Rate Prediction Line
Evaluation of Results . • Compare predicted VO2 to norm table (table 4-8)
Example • Male, Age = 45 • 1st stage yields HR of 98 • 2nd stage yields HR of 121 • 3rd stage yields HR of 143 • Age predicted max HR = 175 • 85% of max HR = 149 • Predicted max = ? Plot to find
Example • Use graph to plot predicted work rate at max HR • Used predicted max work rate for calculation of predicted max VO2 .
Maximal Testing • Purpose • Diagnosis of CAD • Prognosis of client regarding disease • Finding functional capacity for prescription (CRF – Cardiorespiratory Function) • Physician Supervised? • Low risk & men < 45 yr / women < 55 yr • Moderate & High risk
Maximal Testing • Personnel • “Experienced paramedical personnel” • ACSM Exercise Specialist Certified? KSA’s • Exercise Physiology and Related Exercise Science • Pathophysiology and Risk Factors • Health Appraisal, Fitness and Clinical Exercise Testing • Electrocardiography and Diagnostic Techniques • Patient Management and Medications • Medical and Surgical Management • Exercise Prescription and Programming • Nutrition and Weight Management • Human Behavior and Counseling • Safety, injury Prevention, and Emergency Procedures • Program Administration, Quality Assurance, and Outcome Assessment
Maximal Testing • Work Rate Changes • Incremental Format • 1 minute – 3 minutes • Large intensity changes • Time to reach steady state • Ramp Format • ~ 20 sec stages • Small intensity changes • Smoother – non-steady state
Maximal Testing • Clinical • Treadmill • Bruce Protocol • most common • large metabolic demand increments • best for more fit subjects • 3 min stages • increases in speed & grade
Maximal Testing • Clinical • Treadmill • Balke-Ware • small work increments • best for less fit subjects • 1 min stages • speed remains at 3.3 mph • increases in grade only by 1% each stage
Maximal Testing • Sequence of Measures • HR (ECG), BP, RPE, Familiarization, Termination • Box 4-4 • Pre • Exercise • Posttest
Maximal Testing • Indications for Terminating Test • Absolute • Decreased medical status • Equipment Failure • Request to stop • Relative • Change in hemodynamic function • Change in ECG • Fatigue / Chest Pain
Maximal Testing • Symptomatic • Angina Scale • 1+ Light, barely noticeable • 2+ Moderate, bothersome • 3+ Moderately severe, very uncomfortable • 4+ Most severe or intense pain ever experienced • A 3+ would indicate stopping a test
Maximal Testing • Functional Aerobic Impairment • %FAI = (Predicted VO2 – Observed VO2) x 100 Predicted VO2 . . .
Maximal Testing • Metabolic Equivalents – METs • Multiples of VO2 at rest - 3.5 ml/kg/min • Predicted average max VO2 in METs • Men= (57.5 - .445 x age) / 3.5 • Women= (42.3 - .356 x age) / 3.5 . .
Maximal Testing • Performance • Determine functional capacity • Velocity at max for prescription and program assessment • HR at max for prescription and program assessment • Power at max for prescription and program assessment
Maximal Testing • Performance • Methods • Max only • “Quick & dirty” – rapid rise in intensity until max • 8- 12 minutes of testing • No need for steady state • max is goal without fatigue from time
Maximal Testing • Treadmill • Protocol • Ramp or incremental stages • Alternate speed and / or grade • Limitation should be physiological not psychological
Maximal Testing • Cycle Ergometer • Protocol • Ramp or incremental stages • Maintain pedal cadence • Increase tension • Seated & legs only – no standing or arm assistance • Limitation should be physiological not psychological
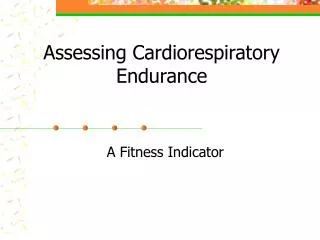
Maximal Testing . • Max VO2 Determination Criteria • Caveat 1. Use of large muscle groups • Caveat 2. Activity specific to “athlete’s” sport • No increase in VO2 with increase in work rate • RER > 1.15 • HR during final stage + 10 beats of predicted HR * Blood lactate concentration > 8 mmoles/liter .
Max VO2 VO2 (ml/kg/min) . Work Rate
Maximal Testing . • PEAK VO2 • Highest VO2 reached without meeting caveats • Highest VO2 reached without meeting 2 of 3 criteria . .
Maximal Testing • Threshold Determination • OBLA – rapid blood lactate accumulation • T-vent - non-linear ventilation increase • Protocol • Smaller intensity increments – not too small! • Even intensity increments • Minute by minute measures – “catch” the inflection point • May last too long to achieve max (fatigue)
Ventilatory Threshold Ventilation (ml/min) T-vent Work Rate
Supra-maximal Testing • Wingate Anaerobic Power Test • Energy supply beyond aerobic metabolism • Protocol • Cycle ergometer • 30 second ride at maximal cadence • Load = 7.5% to 10% of body mass (kg) • Determines peak power (watts) • Determines average power • Determines %Power Decline
Supra-maximal Testing • Wingate Anaerobic Power Test • Indices • Phosphagen stores • Glycolytic system • Buffering capacity • Motivation & capacity to tolerate discomfort • “Kick” at the end of a race or surge during the race • Power to weight ratio (relative power)