Infertility and PCOS
350 likes | 1.08k Vues
Infertility and PCOS. Erinn Myers, M4 Department of Obstetrics and Gynecology University of Tennessee Health Science Center January 28, 2007. Learning Objectives. Following the presentation “Infertility and PCOS ” participants should be able to: Diagnose PCOS.

Infertility and PCOS
E N D
Presentation Transcript
Infertility and PCOS Erinn Myers, M4 Department of Obstetrics and Gynecology University of Tennessee Health Science Center January 28, 2007
Learning Objectives Following the presentation “Infertility and PCOS” participants should be able to: • Diagnose PCOS. • Understand the differences between PCO, PCOS and PCOM. • Decide on possible treatment. • Exclude other problems.
DEFINITION • Inability to conceive after a year of exposure to conception. • Six months > 35 years old. • A disability and a disease…NOT an elective condition. • Great societal and demographic impact
Factors • Male • Ovarian • Cervical • Peritoneal • Tubal • Uterine • Unexplained
Ovulation • An LH (luteinizing hormone) surge occurs 24 to 36 hours prior to ovulation (Follicular rupture = It is the ovary’s job to make a cyst and rupture it.) • Progesterone is increasingly produced after the LH surge • Secretory changes occur in the endometrium due to progesterone.
Ovulation • Pregnancy is absolute proof of ovulation. • Serum progesterones are 99%+ proof of ovulation. These are done: • 8 days after a positive ovulation test • 7 days after ovulation on a monitor • Day 21 and 24 if ovulation day is uncertain.
Ovulation Disorders • PCOS • Hypothyroidism • Hyperprolactinemia • Weight Loss / Weight Gain
PCOS • Diagnosis • Somatic Hyperandrogenism • Lab Hyperandrogenism • Oligo-anovulation • PCOM (polycystic ovarian morphology)
1990 NIH/NICHD • PCOS diagnosis • Ovulatory dysfunction • Clinical hyperandrogenism and/or hyperandrogenemia • Exclusion of other disorders such as • Non-classical adrenal hyperplasia • Androgen secreting tumor • Hyperprolactinemia • Thyroid
2003 ESHRE/ASRM • PCOS diagnosis • At least 2 of the following features • Oligoovulation or anovulation • Clinical and/or biochemical signs of hyperandrogenism • Polycystic ovarian morphology (sonography) • Exclusion of other disorders • 2003 Rotterdam ESHRE/ASRM Consensus. Fertil Steril 81:19, 2004
PCOS • Diagnosis is more clinical than lab. • Androgenism (hirsute, acne, central obesity) • Oligo-anovulatory • PCOM (polycystic ovarian morphology) • Elevated androgens • Androgens decrease with age • Decreased HDL and SHBG
PCOM • PCOM (polycystic ovarian morphology) • > 12 follicles at 2 - 9 mm in at least 1 ovary • Volume > 10cc • Does not apply if on BCPs • If a follicle is >10mm, repeat scan next cycle. • 2003 Rotterdam ESHRE/ASRM Consensus. Fertil Steril 81:19, 2004
PCOM PCOM (polycystic ovarian morphology)
PCOM PCOM (polycystic ovarian morphology)
PCOM vs. Follicles PCOM (polycystic ovarian morphology) vs. Pre- ovulatory Follicles
Screening Tests • FSH and E2 • Prolactin • TSH • 17-OHP • Lipids / HDL decreased • SBHG decreased • 2 hour glucose to screen for diabetes
Exclude • Non-classical 17-hydroxylase deficiency can look like PCOS • HAIRAN - hyperandrogenic insulin resistance and acanthosis nigricans • Adrenal tumor • Cushing’s • Prolactin • Thyroid • Pituitary insufficiency • Hypothalamic amenorrhea
Stop Using • “Inappropriate LH" as a diagnosis • LH / FSH ratio as it is not sufficiently predictive • Fasting insulin as it is not sensitive • Dexamethasone therapy can induce insulin resistance
Utility of LH/FSH Ratio • Study designed to understand the biological variability of the LH/FSH ratio in women with PCOS vs. women with normal menstruation over one full cycle • Will assess the diagnostic utility of the LH/FAH ratio • 10 consecutive blood samples were taken at 4 day intervals in 12 PCOS patients and 11 age and weight matched controls • Cho, LW, et. al. Bio variation of the LH/FSH ratio in normal women and those with PCOS. Endocrine Abstracts (2005) 9 p80
Utility of LH/FSH Ratio • 7.6% of PCOS and 15.6% of controls had LH/FSH ratio above 3 • Sensitivity 7.6% • Specificity 33.7% • Therefore, the biological variation of the LG/FSH ratio is at least as wide in the control group as in the PCOS group • Cho, LW, et. al. Bio variation of the LH/FSH ratio in normal women and those with PCOS. Endocrine Abstracts (2005) 9 p80
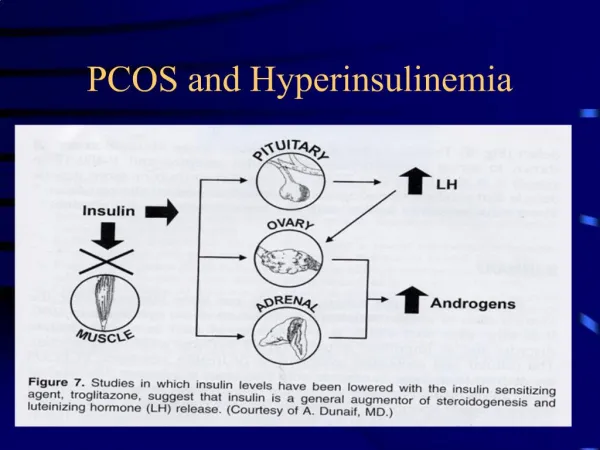
LH/FSH Ratio • Study to determine the incidence of abnormal LH/FSH ratio in women with PCOS with normoinsulinemia and hyperinsulinemia • Access the influence of elevated LH/FSH ratio on selected endocrine and biochemical parameters • LH/FSH ratio119 patients with PCOS was calculated and underwent hormonal and metabolic analysis • Banaszewska B, et. al., Incidence of elevated LH/FSH ration in PCOS women with normo- and hyperinsulinemia. Pocz Acad Med Bialymst. 2003;48:131-4
LH/FSH Ratio • 45.4% had an LH/FSH >2, Normal • 55% had normal gonadotropin ratio • Statistically significant differences between groups with normal and elevated LH/FSH • BMI, serum insulin, LH levels • Majority of women with elevated insulin had a normal LH/FSH ratio • Banaszewska B, et. al., Incidence of elevated LH/FSH ration in PCOS women with normo- and hyperinsulinemia. Pocz Acad Med Bialymst. 2003;48:131-4
LH/FSH Ratio • LH/FSH ratio is not a characteristic attribute of ALL PCOS women • This study found ratio to be elevated <50% • Most of PCOS patients with normal gonadotropin levels also had hyperinsulinemia and obseity • Patients with hyperinsulinemia and elevated LH had increased adrenal androgenic activity • Banaszewska B, et. al., Incidence of elevated LH/FSH ration in PCOS women with normo- and hyperinsulinemia. Pocz Acad Med Bialymst. 2003;48:131-4
PCOS • Treatment • Weight loss and exercise • Clomid (clomiphene citrate) (3 months) • Letrozole (Femara®) (aromatase inhibitor) (3 months) • Metformin (6 months) • Note that the combination of metformin and clomiphene are more productive at months 4-6 compared with months 1-3 . • Gonadotropins
PCOS • Weight loss • Poor results if BMI > 50 • Requires a dedicated program of diet and exercise • Use dieticians who work with diabetics • Liposuction of cutaneous fat is not the same as loss of visceral weight • Richard S. Legro, MD, Penn State College of Medicine, Hershey PCOS PG Course, ASRM, New Orleans, October 2006
PCOS • Medications • BCPs may be better with thin patients that have normal HDL and SHBG • Metformin causes more nausea and weight loss than metformin-XL • Sibutrimine (Meridia ®) – for weight loss • Androgen receptor antagonists for hirsutism • Spironolactone (Aldactone®) and Flutemide (Propecia®) • Ketaconazole (Nizoral®) • Florinithine (Vaniqa®) cream
Letrozole and ClomipheneBirth Defects • There is no increase in birth defects for letrozole or clomiphene if used when not pregnant. • Letrozole associated with fewer birth defects than clomiphene but this is not statistically significant. Tulandi T. Fertil Steril 85:1761, 2006
PCOS • Metformin Therapy – Long Term • Weight • Hyperandrogenism • Increases Fertility • Decreases Cardiac Disease • Decreases Diabetes • Monitor • SHBG (decreased with PCO) • HDL (decreased with PCO) • 2 Hour Glucose
Long Term Management • BCPs may be better with a thin patient and normal HDL and SHBG
Conclusions • PCOS Diagnosis • Somatic or Lab Hyperandrogenism • Oligo-anovulation • Polycystic Ovarian Morphology • Exclude • Non-classical 17-hydroxylase deficiency, HAIRAN, adrenal tumor, Cushing’s, prolactinemia, thyroid disorders, hypothalamic amenorrhea • PCOS Concepts • Decreased HDL and SHBG • LH/FSH ratio is not useful. • Treatment • Weight loss, exercise, clomiphene, aromatase inhibitors, metformin, gonadotropins
Acknowledgement • Dan C. Martin, MD, UTHSC, Memphis • ASRM PCOS Course, New Orleans, 2006