Download
1 / 138
1.41k likes | 2.02k Vues
The MANAGEMENT OF ASTHMA . B. WAYNE BLOUNT, MD, MPH. OBJECTIVES. Define asthma Name the stages of asthma & their respective criteria List the recommended treatment for each stage Describe an action plan Review the recommendations of 3 rd Expert Panel Report (EPR-3)

E N D
The MANAGEMENT OF ASTHMA B. WAYNE BLOUNT, MD, MPH
OBJECTIVES • Define asthma • Name the stages of asthma & their respective criteria • List the recommended treatment for each stage • Describe an action plan • Review the recommendations of 3rd Expert Panel Report (EPR-3) • UNLESS OTHERWISE NOTED, ALL EBM RECOMMENDATIONS ARE FROM COCHRANE
CASE # 1 • 45 Y.O. W MALE C/O COUGH X 3 ½ WEEKS; DAILY, MOSTLY NOCTURNAL
CASE # 1 • Which of the following is NOT in your top 5 differential diagnoses? • A. Post URI Inflammation • B. Post Nasal Drip • C. Allergies • D. Asthma • E. Sinusitis
THE DIFFERENTIAL OF CHRONIC COUGH • POST URI INFLAMMATION • PND • ALLERGIES • ASTHMA • SINUSITIS • GERD • WHAT DO YOU WANT TO DO?
OUR CASE • HX. • P.E.
2. Which of the following is a valid criterion for diagnosing asthma? • A. Wheezing on physical exam • B. Spirometry • C. Symptomatology • D. Sound of the cough
3. Which of the following PFT parameters is MOST likely to be below normal in a patient with asthma? • A. FVC • B. FEV1 • C. TLC • D. FRC
OUR CASE • HIS PFTs : • PARAMETER % PREDICTED • FVC 89 • FEV1 78
4. OUR CASE • We can now diagnose this patient with asthma. • A. True • B. False
REVERSIBILTY OF DEFECT • FEV1 OR PEFR NEEDS TO IMPROVE BY AT LEAST 12%;
THIS MEANS YOU HAVE TO DO PFTs • @ INITIAL ASSESSMENT • AFTER TREATMENT & SX STABILZE • DOCUMENTS “NORMAL” AIRWAY FXN • A MINIMUM OF Q 1-2 YEARS AFTER THAT • WITH EACH EXACERBATION • ‘C’ REC
SPIROMETRY & PEFRs ARE TO ASTHMA AS BLOOD PRESSURE IS TO HYPERTENSION
5. How many stages of asthma severity are there? • A. 3 • B. 4 • C. 5 • D. 6
STAGING THE SEVERITY OF ASTHMA • INTERMITTENT • MILD PERSISTENT • MODERATE PERSISTENT • SEVERE PERSISTENT
INTERMITTENT • SX NIGHT SX LUNG FXN < 2/WK < 2/MO FEV1 or PEF > 80%
MILD PERSISTENT • SX NIGHT SX LUNG FXN • >2/WK BUT > 2/MO FEV1 or PEF > 80% < 1/DAY EXACERBATIONS MAY AFFECT ACTIVITIES
MODERATE PERSISTENT • SX NIGHT SX LUNG FXN DAILY > 1/WK >60% & <80% DAILY USE OF INHALED BETA- AGONIST EXACERBATIONS > 2/WK & AFFECT ACTIVITIES
SEVERE PERSISTENT • SX NIGHT SX LUNG FXN CONTINUAL FREQUENT <60% FREQUENT EXACERBATIONS LIMITED PHYSICAL ACTIVITY
OUR CASE • HOW DO YOU WANT TO TREAT THIS PATIENT & WHY?
6. According to EPR-3, how many age categories are there when considering treatment for asthma? • A. 2 • B. 3 • C. 4 • D. 5
7. According to EPR-3, how many STEPS are there when considering treatment for asthma? • A. 3 • B. 4 • C. 5 • D. 6
EPR-3 • Assess severity before starting Rx • Assess control to guide RX adjustments • 3 age categories for treatment • 6 steps in management to individualize treatment
8. How many known pathophysiologic dysfunctions are in the pathogenesis of Asthma? • A. 1 • B. 2 • C. 3 • D. 4
Asthma Pathophysiology Smooth muscle dysfunction Airway inflammation Airway remodeling Adapted from Bousquet et al. Am J Respir Crit Care Med. 2000;161:1720-1745.
Asthma Pathophysiology Smooth muscle dysfunction • Exaggerated contraction • Increased smooth muscle mass • Increased release of • inflammatory mediators Adapted from Bousquet et al. Am J Respir Crit Care Med. 2000;161:1720-1745.
BRONCHOCONSTRICTION 10 Minutes After Allergen Challenge Before
Asthma Pathophysiology Acute response Chronic inflammatory response • Bronchial hyperreact ivity • Mucosal edema • Airway secretions • Increased inflammatorycell numbers • Epithelial damage Adapted from Bousquet et al. Am J Respir Crit Care Med. 2000;161:1720-1745.
Inflammatory Cells in Lung Tissue E = Epithelium BM = Basement Membrane Laitinen et al. J Allergy Clin Immunol. 1992;90:32-42.
Asthma Pathophysiology Airway remodeling • Cellular proliferation • -smooth muscle cells • -mucous glands • Increased matrix protein deposition • Basement membrane thickening • Angiogenesis Adapted from Bousquet et al. Am J Respir Crit Care Med. 2000;161:1720-1745.
WHAT ARE THE THERAPEUTIC TARGETS? Smooth muscle dysfunction Airway inflammation • lnflammatory cell infiltration/activation • Mucosal edema • Cellular proliferation • Epithelial damage • Basement membrane thickening • Bronchoconstriction • Bronchial hyperreactivity • Hyperplasia/Hypertrophy • Inflammatory mediator release Symptoms/Exacerbations Adapted from Bousquet et al. Am J Respir Crit Care Med. 2000;161:1720-1745.
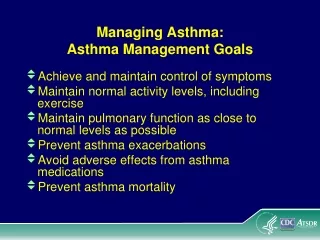
ASTHMA: GOALS OF THERAPY • Control chronic and nocturnal symptoms • Maintain normal activity levels, including exercise • Maintain near-normal pulmonary function • Prevent acute episodes of asthma • Minimize emergency department (ED) visits and hospitalizations • Avoid adverse effects of asthma medications Guidelines for the Diagnosis and Management of Asthma. 1997. NIH Publication No. 97-4051.
TREATMENT • 40 – 50% ARE NOT FOLLOWED CORRECTLY • ‘A’ REC • WRITTEN ACTION PLANS IMPROVE THIS BY A CLINICALLY SIGNIFICANT AMOUNT • ‘B’ REC
THE TREATMENT OF ASTHMA DETERMINED BY CATEGORY OF ASTHMA; A STAGED RESPONSE : • INTERMITTENT • MILD PERSISTENT • MODERATE PERSISTENT • SEVERE PERSISTENT START HIGH AND BACK OFF ‘B’ REC New: 6 steps for the 4 stages
EPR-3’s 6 steps • Step 1 – Intermittent • Step 2 – Mild Persistent • Step 3 – Moderate Persistent • Step 4 – Moderate Persistent • Step 5 – Severe Persistent • Step 6 – Severe Persistent
Stepwise treatment: Ages > 12 years • Step 1 : SABA PRN • Step 2 : Low dose ICS • Step 3 : Low dose ICS & LABA or medium dose ICS • Step 4 : Medium dose ICS & LABA • Step 5 : High dose ICS & LABA; consider Xolair if allergies • Step 6 : High dose ICS & LABA & oral steroids; consider Xolair if allergies
INTERMITTENT • NO DAILY MED NEEDED • USE SHORT-ACTING BETA-AGONIST PRN SX. • EDUCATE : • ASTHMA • MDI USE • SELF MANAGEMENT • ACTION PLAN • ENVIRONMENTAL CONTROL MEASURES
MILD PERSISTENT • A CONTROLLER MED : • INHALED STEROID IS PREFERRED • A CROMONE MAY SUFFICE IN SOME • UNCOMMON: LTM • RARE: THEOPHYLLINE • RESCUE MED : • INHALED BETA-AGONIST • EDUCATION
MODERATE PERSISTENT • INCREASE STEROID (MEDIUM DOSE) • ADD LONG-ACTING BETA-AGONIST* • ADD LTM • CONTINUE RESCUE MED & EDUCATION *CONTROVERSIAL
SEVERE PERSISTENT • HIGH DOSE INHALED STEROID • LABA • SYSTEMIC STEROID • LTM • THEOPHYLLINE • RESCUE MED(S) • INTENSIFY EDUCATION • “WHATEVER IT TAKES”
SO OUR PATIENT HAS _____ • AND WE WILL USE WHAT MED(S) FOR HIM? • GO BACK TO HIS SX & PFTs
MUST TEACH MDI USE • TELL • DEMONSTATE • WATCH • ASSESS
TRICKS WITH USING MDIs ? • RINSE MOUTH ‘B’ REC • NEBS VS. CHAMBERS ‘A’ REC
KNOWLEDGE OF AND PRACTICAL SKILLS WITH THE DEVICES 75 67* RT RN 48 MD MeanKnowledgeScore(%) 50 39 25 0 n = 30 n = 30 n = 30 *P<0.0001 vs RN and MD Hanania et al. Chest. 1994;105:111-116.
MEDICAL STAFF’S ABILITY TO EFFECTIVELY DEMONSTRATE PROPER INHALER TECHNIQUES RT 98* 97* 100 RN 82 78 MD 80 69 Mean DemonstrationScore (%) 60* 57 60 40 21 20 12 0 MDI Turbuhaler® MDI + AeroChamber® *P<0.0001 vs RN and MD Hanania et al. Chest. 1994;105:111-116.