Download
1 / 55
560 likes | 613 Vues
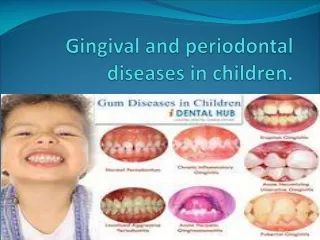
Gingival enlargement associated with systemic diseases. Contents. Introduction Terminologies Classification of gingival enlargements Gingival enlargement associated with systemic diseases and their clinical & Histopathological features Diagnosis Management of gingival enlargement

E N D
Gingival enlargement associated with systemic diseases
Contents Introduction Terminologies Classification of gingival enlargements Gingival enlargement associated with systemic diseases and their clinical & Histopathological features Diagnosis Management of gingival enlargement Recurrence of gingival enlargement Conclusion
Introduction Accepted current terminology for this condition is gingival enlargement and gingival overgrowth. These are strictly clinical descriptive terms and to avoid the erroneous pathologic connotations of terms used in the past such as hypertrophic gingivitis or gingival hyperplasia. Gingival enlargement is the overgrowth of the gingiva characterized by an expansion and accumulation of the connective tissue with occasional presence of increased number of cells. It is caused by several factors, such as, inflammation, leukemia, drugs and inheritance.
Terminologies • Gingival Enlargement: An overgrowth or increase in size of the gingiva • Gingival Hyperplasia: An enlargement of the gingiva due to an increase in the number of cells • Gingival Hypertrophy: An enlargement of the gingiva due to an increase in the size of cells (According to the Glossary of Periodontal Terms, 4th Edition, 2001)
CLASSIFICATION I. Inflammatory enlargement A. Chronic B. Acute II. Drug-induced enlargement III. Enlargements associated with systemic diseases A. Conditioned enlargement Pregnancy Puberty Vitamin C deficiency Plasma cell gingivitis Nonspecific conditioned enlargement (granulomapyogenicum) B. Systemic diseases causing gingival enlargement Leukemia Granulomatous diseases (Wegener’s granulomatosis, Sarcoidosis etc.) IV. Neoplastic enlargement (gingival tumors) A. Benign tumors B. Malignant tumors V. False enlargement
Based on location and distribution • Localized • Generalised • Marginal • Papillary • Diffuse • Discrete
Gingival enlargement associated with systemic diseases Many systemic diseases can develop oral manifestations that may include gingival enlargement These systemic diseases and/or conditions can affect the periodontium by two different mechanisms as follows: • Magnification of an existing inflammation initiated by dental plaque • Manifestation of the systemic disease independently of the inflammatory status of the gingiva
Conditioned Enlargement • Conditioned enlargement occurs when the systemic condition of the patient exaggerates or distorts the usual gingival response to dental plaque • The 3 types of conditioned gingival enlargement are- • Hormonal (pregnancy, puberty) • Nutritional (associated with vitamin C deficiency) • Allergic
Enlargement in Pregnancy: • During pregnancy there is an increase in levels of both progesterone and estrogen, which induce changes in vascular permeability, leading to gingival edema and an increased inflammatory response to dental plaque.
Why?????????? • The estrogen receptors such as ER-α and ER-β are present on the vascular smooth muscles which causes smooth muscle relaxation and results in vasodilation. • The estrogen causes increased levels of Vascular endothelial growth factor which is a potent stimulator of microvascular permeability. • Progesterone induces vascular permeability by formation of gaps in the normally intact endothelial lining.
Susceptibility to infections (e.g. periodontal infection) increases during early gestation due to • Suppression of T-cell activity • Decreased neutrophilchemotaxis and phagocytosis, • Altered lymphocyte response • Depressed antibody production • Chronic maternal stress • Down regulation of IL-6 production, rendering the gingiva less efficient at resisting the inflammatory challenges produced by the bacteria • decreased levels of immunoglobulin G (IgG)
Marginal enlargement- • The enlargement is usually generalized and tends to be more prominent interproximally • The enlarged gingiva is bright red or magenta, soft, and friable, and has a smooth, shiny surface Tumorlike Gingival Enlargement- • The so-called pregnancy tumor is not a neoplasm. • It usually occurs after the third month of pregnancy but may occur earlier
A heightened gingival response to plaque during pregnancy results in pregnancy-associated gingivitis
Localized gingival enlargement in a 27-year old pregnant patient…
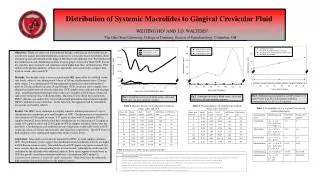
Microscopic view of gingival enlargement in pregnant patient showing abundance of blood vessels and interspersed inflammatory cells…
Enlargement in Puberty: • It is seen sometimes during puberty in both male and female adolescents and appears in areas of plaque accumulation • The enlargement is marginal and interdental and is characterized by prominent bulbous interproximal papillae • The degree of enlargement and the tendency to develop massive recurrence in the presence of relatively scant plaque deposits distinguish pubertal gingival enlargement from uncomplicated chronic inflammatory enlargement
Tiainenet al. [1992] showed that the severity of puberty gingivitis was related more closely to plaque build up than to hormones.
Conditioned gingival enlargement in puberty in a 13-year old boy…
Enlargement in Vitamin C Deficiency: • Acute vit C deficiency itself does not cause gingival inflammation, but it does cause hemorrhage, collagen degeneration, and edema of the gingival connective tissue • The enlargement is marginal; the gingiva is bluish-red, soft and friable and has a smooth, shiny surface
Plasma Cell Gingivitis: • Also called Atypical gingivitis and Plasma cell gingivostomatitis • Plasma cell granuloma- Bhasker 1988 • Plasma cell gingivitis is thought to be allergic in origin, possibly related to components of chewing gum, dentifrices, or various diet components • Often shows a mild marginal gingival enlargement, that extends to the attached gingiva • The gingiva appears soft, friable, and sometimes granular and bleeds easily
Plasma cell gingivitis… In a case report of PCG, PCG associated with generalized aggressive periodontitis (GAgP), which was brought on by the use of herbal toothpaste containing “Acacia” extract from the tree “Acacia Arabica.” Anjali makkar, JISP, 2013 Jul-Aug; 17(4): 527–530.
Nonspecific Conditioned Enlargement (PyogenicGranuloma): • The lesion varies from a discrete, spherical, tumor like mass with a pedunculated attachment to a flattened, keloid like enlargement with a broad base
Why???????????? • Oral pyogenic granuloma arises as a result of some minor trauma to the tissues that provide a pathway for invasion of nonspecific types of microorganisms. • The tissues responds to these organisms of low virulence by the overzealous proliferation of a vascular type of connective tissue. • Ainamo suggested that trauma can cause release of various endogenous substances including angiogenic factors from the tumor cells and it may also cause disturbances in the vascular system of the affected area.
Systemic Diseases That Cause Gingival Enlargement • Several systemic diseases may result in gingival enlargement through different mechanisms • These are usually uncommon cases • Leukemia • Granulomatous diseases: • Wegener’s Granulomatosis • Sarcoidosis
Leukemia Leukemia, like other cancers, results from mutations in the DNA. Certain mutations can trigger leukemia by activating oncogenes or deactivating tumor suppressor genes, and thereby disrupting the regulation of cell death, differentiation or division. These mutations may occur spontaneously or as a result of exposure to radiation or carcinogenic substances
In leukemia typically the lamina propria is densely packed with leukemic cells extending from the basal cell layer of the epithelium into the gingiva, there by altering the normal anatomy. Regional blood vessels are compressed by infiltration
Granulomatous Diseases • Wegener's Granulomatosis Charecterised by a triad of necrotic vasculitis, necrotic glomerulonephritis and granulomatous inflammation of the upper or lower respiratory tract Anti-neutrophilcytoplasmic antibodies (ANCA) to the cytoplasmic antigens of neutrophil granulocytes
Sarcoidosis • Tuberculousis associated gingival enlargement VaradhanKarthikeyanin 2006 has reported a rare case of diffuse gingival enlargement in a patient with primary tuberculosis.
Syndromes typically associated with gingival enlargements: Apert’s syndrome: • Apert’ssyndrome is a form of acrocephalosyndactyly • Apert’s syndrome occurs as a result of androgen end organ hyper-response affecting the epiphyses and sebaceous glands that results in early epiphyseal fusion leading to short stature, short and fused digits and acrocephaly. Premalathaet al; JISPP: 2010, issue 4, vol 28
The oral cavity of Apert patients includes a reduction in the size of the maxilla, tooth crowding, anterior open-bite of the maxilla, impacted teeth, delayed eruption, ectopic eruption, supernumerary teeth, and thick gingiva. The mandible usually is within normal size and shape, and simulates a pseudoprognathism clinical and radiographic features and case report: Felipe PaesVaroliet al, Rev OdontoCienc 2011
Cross–McKusick–Breen syndrome • also known as "Cross syndrome," "Hypopigmentation and microphthalmia," and "Oculocerebral-hypopigmentation syndrome“ • extremely rare disorder characterized by white skin, blond hair with yellow-gray metallic sheen, small eyes with cloudy corneas, jerky nystagmus, gingival fibromatosis and severe mental and physical retardation. • It was characterized in 1967
Melkersson-Rosenthal Syndrome: • Melkersson-Rosenthal syndrome (MRS) is a very rare neurological disorder. • The origin of MRS is as yet unknown. • The diagnosis of the disease usually occurs in the patient’s second or third decade of life. • The clinical symptoms are remittent swellings of the oral, pharyngeal and laryngeal mucosa as well as the lips. Due to the presence of granulomata in all orofacial soft tissues, a plicated tongue as well as facial nerve paralysis may occur. Intermittent increase of mucosal swelling, including swelling of the gingiva, may increase the risk of development of chronic periodontitis by inhibiting local plaque removal.
Generalised swelling and hypoplastickeratinisation of the gingiva. Chronic Periodontitis in Conjunction with Melkersson-Rosenthal Syndrome: A Case Report and Literature Review: Frank Broseler, Angelika Neuber: Perio 2006; Vol 3, Issue 1: 43–48.
Sturge weber syndrome • Sturge Weber syndrome (SWS) was first described by Schirmer in 1860 and later more specifically by Sturge in 1879 • Most common features are epilepsy, Port-wine stain and dermal angiomas, abnormal findings in skull radiographs, mental retardation, ocular involvement and hemiplegia. the most common feature is a gingival hemangiomatous lesion usually restricted to ipsilateral maxilla, mandible, floor of mouth, lips, cheeks, palate and tongue. A Case Report NehaKhambeteet al INTERNATIONAL JOURNAL OF DENTAL CLINICS Vol 3 JAN-MAR 2011 • Oral changes occur in 40% cases of this syndrome and may include massive growth of the gingiva and asymmetric jaw growth. Sturge-Weber syndrome: A case report MUKHOPADHYAY S. J Indian SocPedod Prevent Dent - Supplement 2008.
MANAGEMENT OF GINGIVAL ENLARGEMENTS • Gingivectomy using scalpel The dotted line represents the external bevel incision, and the shaded area corresponds to the tissue to be excised. Gingivectomy incision may not remove the entire hyperplastic tissue (shaded area) and may leave a wide wound of exposed connective tissue.
Flap technique A, Initial reverse bevel incision followed by thinning of the enlarged gingival tissue; dotted lines represent incisions, and the shaded area represents the tissue portion to be excised. B, After flap elevation, enlarged portion of the gingival tissue is removed. C, The flap is placed on top of the alveolar bone and sutured.
Ledge and Wedge and Internal Bevel Gingivectomy Techniques A, Preoperative diagram showing gingival enlargement. B, The initial facial and lingual incisions (1) are made perpendicular to the gingiva to strike the base of the soft tissue pockets. C,Secondary incisions (2) are made on the facial and lingual at a 45-degree external bevel to remove the remaining soft tissue ledges. D, Postoperative result.
Gingivectomy using electrocautery COAG -20-30 (25)W Blend-Cut -20-30 W
Advantages Disadvantages Unpleasant odor. When the bone touches it causes necrosis. The heat generated causes loss of periodontal support when the electrode is used to close to bone. Causes cementum burns The smoke is considered a mild carcinogen. • Electrosurgery is thought of as the sculpture of living tissue because it works without pressure, unlike scalpel. • Bleeding is controlled by electrosurgery. • Adjunct to other therapies due to its ability to induce heat in fluid. For eg: accelerating desensitizing agents, in gingival curettage, in root canal sterilization, accelerating whitening agents in spot whitening.
Gingivectomy using laser • CO2 laser -7-W of power continuous wave mode. • Er:YAG laser -3 W of power continuous wave mode • Nd:YAG laser- 4 W of power continuous wave mode • diode laser- 2 W of power continuous wave mode
Relative bloodless operative and post-operative field • Greater accuracy in making incisions • Sterilization of the operating field • Minimal swelling and scarring • Less post-operative pain • Hemostasis
TREATMENT OF LEUKEMIC GINGIVAL ENLARGEMENT • Bleeding & clotting times and platelet count of the patient should be checked and the hematologist consulted before periodontal treatment • The enlargement is treated by scaling and root planing carried out in stages under topical anesthesia. • The initial treatment consists of gently removing all loose accumulations with cotton pellets. • Progressively deeper scalings are carried out at subsequent visits. • Antibiotics are administered systemically the evening before and for 48 hours after each treatment to reduce the risk of infection
TREATMENT OF GINGIVAL ENLARGEMENT IN PREGNANCY • Treatment requires elimination of all local irritants responsible for precipitating the gingival changes in pregnancy • Marginal and interdental gingival inflammation and enlargement are treated by scaling and curettage. • Treatment of tumor-like gingival enlargements consists of surgical excision and scaling and planing of the tooth surface. In pregnancy, the emphasis should be on- • Preventing gingival disease before it occurs • Treating existing gingival disease before it worsens
TREATMENT OF GINGIVAL ENLARGEMENT IN PUBERTY • Gingival enlargement in puberty is treated by performing scaling and curettage, removing all sources • The use of escharotic drugs has been recommended in the past for the removal of gingival enlargements of irritation, and controlling plaque.