Download
1 / 31
310 likes | 352 Vues
Physiology and promotive health B.SC iiiRD sEM. Contents : Blood- composition and function. Blood group and related diseases. Heart : functions and functioning of heart. Bhavneet Kaur Physiology Lecturer Govt Home Science college Sector 10 Chandigarh. BLOOD

E N D
Physiology and promotive health B.SC iiiRDsEM Contents : Blood- composition and function. Blood group and related diseases. Heart : functions and functioning of heart. BhavneetKaur Physiology Lecturer Govt Home Science college Sector 10 Chandigarh
BLOOD • Blood is a highly specialized circulating tissue consisting of several types of cells suspended in a fluid medium known as plasma. • Blood contain both extracellular fluid (the fluid in plasma) and intracellular fluid (the fluid in the red blood cells). However, blood is considered to be a separate fluid compartment because it is contained in a chamber of its own, the circulatory system. • The average blood volume of adults is about 7 % of body weight or about 5 litres. About 60% of blood is plasma and 40 % is red blood cells, but these percentages vary considerably depending on gender, weight and other factors.
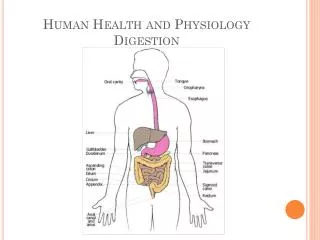
FUNCTIONS OF BLOOD Since blood is a circulating fluid and almost every organ receives a blood supply, it performs a number of vital functions in the body which are as follows: • RESPIRATION: Transport of oxygen from the lungs to different tissues, and the transport of carbon dioxide from the tissues to lungs is mainly effected by blood. • TRANPORT OF FOOD MATERIALS: Blood is the only medium by means of which the absorbed food materials are transported. • EXCRETION: Metabolic wastes like urea, uric acid, creatinine, water, carbon dioxide, etc., are transported by blood, to kidney, lungs, skin and intestine for removal. • REGULATION OF BODY TEMPERATURE: Blood distributes heat generated in the muscles by the oxidation of carbohydrates and fats, throughout the body. • MAINTENANCE OF ACID-BASE BALANCE: The blood has buffering capacity and maintains normal acid-base balance in the body.
REGULATION OF WATER BALANCE: Water balance between blood and tissues fluid. • DEFENSE: Blood affords protection to the body against infections and forgine antigen and antibodies . • TRANSPORT OF HORMONES AND METABOLITES: Blood serves as a medium to distribute hormones, chemicals and essential metabolites to different parts of the body. • COAGULATION: It is part of body’s self-repair mechanism. COMPONENTS OF BLOOD PLASMA: It is a pale yellow or gray yellow, slightly alkaline , somewhat viscous fluid has a constant chemical composition. The various components of plasma are: Water : 90 % Inorganic Salts : 1 % Proteins : 7 - 8% Food materials, waste products, dissolved gasses , regulatory substances( vitamins, hormones, enzymes, anticoagulants, choleterol and antibodies ). : 1%
FUNCTIONS/PROPERTIES OF PLASMA PROTEINS • RAW MATERIAL : plasma proteins act as a source of proteins for the tissue cells which may synthesize their own proteins from them. • BUFFERS : The plasma proteins act as buffers by virtue of their power of H ion acceptance , but they account for less than 1/6 th of the total buffering power of the blood. These plasma proteins as aminoacids serve as acid- base buffers. They maintain pH of the blood by combining with acids and bases. • OSMOTIC PRESSURE : The plasma protein normally have an osmotic pressure of 25mm.Hg and thus influence the exchange of fluid between blood and tissue. • TRANSPORT : Plasma proteins transport certain materials in combination with them. For Example: Thyroxine and Vitamin B12 are bound to α- globulin. Lipids are bound to β- globulin. • VISCOSITY : The viscosity of the blood is a factor in maintaining the peripheral resistance and thereby , the arterial blood pressure. This viscosity of a protein solution depends far more on the shape of the protein than on its size.
RED BLOOD CELLS OR ERYTHROCYTES. A unique feature of the RBCs is the presence of a red, iron containing , oxygen carrying pigment, the hemglobin They are confined to the blood. They are lacking in the lymph and tissue fluid. The size of RBC are 7-8 ųm in diameter and 2 ųm thick near the rim. There are 600 RBC to every one WBC. A normal healthy adult man and women have 5 and 4.5 million RBC s /mm³ of blood respectively. The new born has higher no of RBC. The increase in count of RBC is called Polycythemia which is seen during exercise to meet the increased demand of oxygen and at high altitudes. Human RBC has a life span of 120 days. About 2 to 10 million RBC s are destroyed every second in human being. The portion of aminoacid breaks down into its constitutional amino acids whereas iron of the haem portion is extracted and stored I the liver as ferritin. Excess RBC’s are stored in spleen. ERYTHROPOIESIS : Formation of red blood corpuscles is called erythropoiesis. It occurs in liver and mesenchyme in early fetus, in spleen and bone marrow in late fetus, in red bone marrow of long bones in the children, and red bone marrow of skull, ribs, sternum an vertebrae in the adults. It is controlled by feed back mechanism.
LEUCOCYTES or WHITE BLOOD CELLS GranulocytesAgranulocytes (3 types) (2 types) 1 Eosinophils 1 Lymphocytes 2 Basophils 2 Monocytes 3 Neutrophils
GRANULOCYTES : are characterized by the presence of granules in their cytoplasm. They are also called polymorphonuclear leukocytes (PMN or PML) because of the varying shapes of the nucleus which is usually lobed into three segments. Granulocytes are released from the bone marrow by the regulatory complement proteins • EOSINOPHILS : (2-6%) They have bilobed nucleus, play role in allergic reactions and parasitic infections , their number increase sharply in certain diseases. Eosinophils are cytotoxic ( chemicals that inhibit or prevent normal physiology of a cell). They take acidic strains. • BASOPHILS : (0-2%) They take basic strain, lowest in number, their number increases during infections, have S shaped nucleus. Basophiles get converted into mast cells which secrete histamine ,involved in allergic reactions.Histamine causes dilation and increased permeability of capillaries close to the basophil. Injured basophils and other leukocytes will release another substance called prostaglandins that contributes to an increased blood flow to the site of infection. Both of these mechanisms allow blood clotting elements to be delivered to the infected.
NEUTROPHILS : ( 60-70% ) They have multilobed nucleus, takes neutral strains, play role in specific immunity. Neutrophils are phagocytes they are ferocious eaters and rapidly engulf invaders coated with antibodies and complement and damaged cells or cellular debris. Neutrophils do not return to the blood, they turn into pus cells and die. • AGRANULOCYTES : They have relatively clear cytoplasm. • LYMPHOCYTES: (20-30%) They have rounded nucleus, provide specific immunity. B Lymphocytes: These are responsible for making antibodies. T Lymphocytes: There are 3 subsets of these: 1.Inflammatory T cells: that recruit macrophages and neutrophils to the site of infection or other tissue damage. 2.Cytotoxic T Lymphocytes: kills virus-infected and tumor cells. 3.Helper T cells: enhances the production of antibodies by B cells. • MONOCYTES: (2-8%) They are maximum in size. They leave blood and become macrophages. They provide non specific immunity.
PLATELETS Platelets, also called thrombocytes, They are not true cells. They are fragments of big cells called magakaryocytes. They are present in bone marrow and split into small fragments called platelets. Their production is regulated by the hormone called Thrombopoietin. The sticky surface of the platelets allow them to accumulate at the site of broken blood vessels to form a clot. This aids in the process of hemostasis ("blood stopping"). Platelets secrete factors that increase local platelet aggregation. Tissue Thromboplastin- clotting factor released by injured tissue . This tissue thromboplastininnitiates the process of clotting. This will convert Prothrombin Thrombin .Prothrombin is an inactivate form of thrombin. Thrombin converts Fibrinogen Fibrin. Fibrin threads will forms a mesh/network with it platelets are attached and form a clot.
ABO BLOOD GROUP SYSTEM • The ABO blood group system is the most important blood type system (or blood group system) in human blood transfusion. The associated anti-A antibodies and anti-B antibodies are usually IgM antibodies, which are produced in the first years of life by sensitization to environmental substances such as food, bacteria and viruses. The ABO blood group system discovered by the Austrian scientist Karl Landsteiner in 1900. The ABO locus is located on chromosome 9. The H antigen is an essential precursor to the ABO blood group antigens. The H locus is located on chromosome 19. The ABO locus has three main alleleic forms: A, B, and O. The A allele encodes a glycosyltransferase that bonds α-N-Acetylgalactosamine to D-galactose end of H antigen, producing the A antigen. The B allele encodes a glycosyltransferasethat joins α-D-galactose bonded to D-galactose end of H antigen, creating the B antigen. The O allele differs slightly from the A allele by deletion of a single nucleotide – Guanine at position 261. This results in H antigen remaining unchanged in case of O groups.
Due to the presence of isoantibodies against non self blood group antigens, individuals of type A blood group immediately raises anti-B antibodies against B-blood group RBCs if transfused with blood from B group. The anti-B antibodies bind to B antigens on RBC and causes complement-mediated lysis of the RBCs. The same happens for B and O groups (which raises both anti-A and anti-B antibodies). However only blood group AB does not have anti-A and anti-B isoantibodies. Hence they can receive blood from all groups and are universal recipient. • Individuals with type A blood can receive blood from donors of type A and type O blood. • Individuals with type B blood can receive blood from donors of type B and type O blood. • Individuals with type AB blood can receive blood from donors of type A, type B, type AB, or type O blood. • Individuals with type O blood can receive blood from donors of only type O. • Individuals of type A, B, AB and O blood can receive blood from donors of type O blood. Type O- blood is called the universal donor. • Type O carries anti-A and anti-B antibodies in the serum. To transfuse a type A, B, or AB recipient with type O whole blood would produce a hemolytic transfusion reaction due to the antibodies found in the serum of whole blood. .
No antibodies are formed against the H antigen, except in those individuals with the Bombay phenotype. • Blood groups are inherited from both parents. The ABO blood type is controlled by a single gene (the ABO gene) with three alleles: i, IA, and IB. • The IA allele gives type A, IB gives type B, and i gives type O. As both IA and IB are dominant over i, only ii people have type O blood. Individuals with IAIA or IAi have type A blood, and individuals with IBIB or IBi have type B. IAIB people have both phenotypes, because A and B express a special dominance relationship: codominance, which means that type A and B parents can have an AB child. A type A and a type B couple can also have a type O child if they are both heterozygous (IBi,IAi) • Subgroups of type A A1 and A2 • The A blood type contains about twenty subgroups, of which A1 and A2 are the most common (over 99%). A1 makes up about 80% of all A-type blood, with A2 making up the rest. These two subgroups are interchangeable as far as transfusion is concerned, however complications can sometimes arise in rare cases when typing the blood.
RH BLOOD GROUP SYSTEM • It is the clinically most important blood group system besides ABO. The Rh blood group system currently consists of 50 defined blood group antigens among which the 5 antigens D, C, c, E, and e are the most important ones. The commonly used terms Rh factor, Rh positive and Rh negative refer to the D antigen only. Besides its role in blood transfusion, the Rh blood group system, in particular the strongest D antigen, is a relevant cause of the hemolytic. Individuals either have, or do not have, the "Rh factor" on the surface of their red blood cells. This term strictly refers only to the most immunogenic D antigen of the Rh blood group system. This is usually indicated by Rh positive (does have the D antigen) or Rh negative (does not have the D antigen). The main antigens are D, C, E, c and e, which are encoded by two adjacent gene loci, the RHD gene which encodes the RhD protein with the D antigen (and variants) and the RHCE gene which encodes the RhCE protein with the C, E, c and e antigens (and variants). There is no d antigen. Lowercase "d" indicates the absence of the D antigen (the gene is usually deleted or otherwise nonfunctional).
DISEASES ASSOCIATED WITH BLOOD GROUPS • HEMOLYTIC DISEASE OF THE NEWBORN OR RH INCOMPATIBILITY :This condition occurs when there is an incompatibility between the blood types of the mother and the fetus. These terms do not indicate which specific antigen-antibody incompatibility is implicated. The disorder in the fetus due to Rh D incompatibility is known as erythroblastosisfetalis. • When the condition is caused by the Rh D antigen-antibody incompatibility, it is called Rh D Hemolytic disease of the newborn. Here, sensitization to Rh D antigens (usually by feto-maternal transfusion during pregnancy) may lead to the production of maternal IgG anti-D antibodies which can pass through the placenta. This is of particular importance to D negative females of or below childbearing age, because any subsequent pregnancy may be affected by the Rhesus D hemolytic disease of the newborn if the baby is D positive. The vast majority of Rh disease is preventable in modern antenatal care by injections of IgG anti-D antibodies (Rho(D) Immune Globulin).
ABO HEMOLYTIC DISEASE OF THE NEWBORN :ABO blood group incompatibilities between the mother and child does not usually cause hemolytic disease of the newborn (HDN) because antibodies to the ABO blood groups are usually of the IgM type, which do not cross the placenta; however, in an O-type mother, IgG ABO antibodies are produced and the baby can develop ABO hemolytic disease of the newborn. • THALASSAEMIA :is an inherited autosomal recessive blood disease. In thalassemia, the genetic defect results in reduced rate of synthesis of one of the globin chains that make up hemoglobin. Reduced synthesis of one of the globin chains can cause the formation of abnormal hemoglobin molecules, thus causing anemia, the characteristic presenting symptom of the thalassemias. Hemoglobinopathies imply structural abnormalities in the globin proteins themselves. The two conditions may overlap, however, since some conditions which cause abnormalities in globin proteins (hemoglobinopathy) also affect their production (thalassemia). Thus, some thalassemias are hemoglobinopathies, but most are not. Either or both of these conditions may cause anemia.
SICKLE-CELL DISEASE :or sickle-cell anaemia is a genetic life-long blood disorder characterized by red blood cells that assume an abnormal, rigid, sickle shape. Sickling decreases the cells' flexibility and results in a risk of various complications. The sickling occurs because of a mutation in the haemoglobin gene. Life expectancy is shortened, with studies reporting an average life expectancy of 42 and 48 years for males and females, respectively. • Sickle-cell anaemia is the name of a specific form of sickle-cell disease in which there is homozygosity for the mutation that causes HbS. Sickle-cell anaemia is also referred to as "HbSS", "SS disease", "haemoglobin S" or permutations thereof. In heterozygous people, who have only one sickle gene and one normal adult haemoglobin gene, it is referred to as "HbAS" or "sickle cell trait". Other, rarer forms of sickle-cell disease include sickle-haemoglobin C disease (HbSC), sickle beta-plus-thalassaemia (HbS/β+) and sickle beta-zero-thalassaemia (HbS/β0). • HAEMOPHILIA : is a group of hereditary genetic disorders that impair the body's ability to control bloodclotting or coagulation, which is used to stop bleeding when a blood vessel is broken. Haemophili A (clotting factor VIII deficiency) is the most common form of the disorder, occurring at about 1 in 5,000–10,000 male births.
The heart is a specialised muscle that contracts regularly and continuously, pumping blood to the body and the lungs. The pumping action is caused by a flow of electricity through the heart that repeats itself in a cycle. If this electrical activity is disrupted - for example by a disturbance in the heart's rhythm known as an 'arrhythmia' - it can affect the heart's ability to pump properly. • The heart's natural pacemaker - the SA node - sends out regular electrical impulses from the top chamber (the atrium) causing it to contract and pump blood into the bottom chamber (the ventricle). The electrical impulse is then conducted to the ventricles through a form of 'junction box' called the AV node. The impulse spreads into the ventricles, causing the muscle to contract and to pump out the blood. The blood from the right ventricle goes to the lungs, and the blood from the left ventricle goes to the body. • The heart has four chambers - two at the top (the atria) and two at the bottom (the ventricles). The normal trigger for the heart to contract arises from the heart's natural pacemaker, the SA node, which is in the top chamber (see the diagram, right). The SA node sends out regular electrical impulses causing the atrium to contract and to pump blood into the bottom chamber (the ventricle). The electrical impulse then passes to the ventricles through a form of 'junction box' called the AV node (atrio-ventricular node). This electrical impulse spreads into the ventricles, causing the muscle to contract and to pump blood to the lungs and the body.
The electrical activity of the heart can be detected by doing an 'electrocardiogram' (also called an ECG). An ECG recording looks something like the one shown below. • There are four heart valves. They are all one-way valves to keep blood moving through the various chambers of the heart. • The mitral valve guards the opening between the atrium and the ventricle in the left side of the heart. It allows blood to flow forward from the atrium to the ventricle, and prevents blood from flowing backwards. The mitral valve has tiny cords attached to the walls of the ventricles. This helps support the valve’s small flaps or leaflets. • The aortic valve, also called a semi-lunar valve, has three segments that prevent the return of the blood from the aorta to the left ventricle. It looks like three half Ping-Pong balls. Valves on the heart’s left side need to withstand much pressure. Sometimes they wear out and leak or become thick and stiff.
The pulmonary valve is located at the junction of the pulmonary artery and the right ventricle. When the right ventricle contracts, the pulmonary valve opens, forcing the blood into the artery which leads to the lungs. It is also a semi-lunar valve. When the chamber relaxes, this valve closes and prevents a backflow of the blood. • The tricuspid valve is located between the upper and lower chamber in the right side of the heart. Its position corresponds to the mitral valve in the left side of the heart.
CARDIAC CYCLE • The heart has an increasing rhythmic activity. It pumps blood by its contraction and relaxation. The contraction of the heart is called systole and the relaxation is called diastole. The contraction and relaxation together constitute the heart beat. The heart beats at the rate of 72 beats per minute. The changes that occur in the heart during the beat one is repeated in the same order in the next beat. This cyclical repetition is called cardiac cycle. During the cardiac cycle, blood flows through the cardiac chambers in a specific manner and direction, the backward flow being prevented by the valves. There are 3 main events in the cardiac cycle, namely a) Auricular systole b) Ventricular systole c) Joint diastole
AURICULAR SYSTOLE : This phase involves the contraction of the 2 auricles, pushing the blood into the respective ventricles. There is no back flow of blood due to the presence of the bicuspid and the tricuspid valves. The atrial systole takes 0.1 second. This is followed by the atrial diastole when both the auricles relax simultaneously. This is about 0.7 seconds. • VENTRICULAR SYSTOLE: This takes place alongside auricular diastole. The pressure on the blood in the ventricles increases. The auriculo ventricular valves close rapidly to prevent the backward flow of blood into the auricles. This closing of the auriculo ventricular valves at the start of ventricular systole produces first heart sound called lubb. • As the pressure in the ventricle increases, than that in the great arteries, namely pulmonary artery and the aorta, the semilunar valves guarding the openings of these arteries open and blood enters them. From the right ventricle, the deoxygenated blood enters the pulmonary artery. From the left ventricle, the oxygenated blood enters the dorsal aorta, to be taken to all body parts. Ventricular systole takes about 0.3 seconds.
JOINT DIASTOLE :Ventricular systole is followed by ventricular diastole. The auricles are already in diastole, so all the chambers of the heart are in diastole. When the ventricles are in diastole, the pressure in the ventricles decreases more than that in the great arteries. So to prevent the backward flow of blood, the semilunar valves close rapidly. This produces the second heart sound called dup. • During a complete cardiac diastole, blood from the superior and inferior vena cava flows into the auricles slowly. The pressure in the ventricles decreases and finally becomes lower than atrial pressure. Then the AV values open and blood (auriculo ventricular valves) from the atria starts entering into the relaxing ventricles. A complete cardiac diastole takes only 0.4 seconds. An entire cardiac cycle is completed in 0.8 seconds.
Heart DiseasesAtherosclerosis: Narrowing of the lumen of the artery
MYOCARDIAL INFARCTION (MI) or acute myocardial infarction (AMI), commonly known as a heart attack, is the interruption of blood supply to part of the heart, causing some heart cells to die. This is most commonly due to occlusion (blockage) of a coronary artery following the rupture of a vulnerable atherosclerotic plaque, which is an unstable collection of lipids (fatty acids) and white blood cells (especially macrophages) in the wall of an artery. The resulting ischemia (restriction in blood supply) and oxygen shortage, if left untreated for a sufficient period of time, can cause damage or death (infarction) of heart muscle tissue (myocardium). • Symptoms of acute myocardial infarction include sudden chest pain (typically radiating to the left arm or left side of the neck), shortness of breath, nausea, vomiting, palpitations, sweating and anxiety (often described as a sense of impending doom).