Download
1 / 19
190 likes | 387 Vues
A Public Health Insurance Plan:. Reducing Costs & Improving Quality. Health Care Reform Should Expand Consumer Choice. We should be able to keep our employer-provided coverage if we like it.

E N D
A Public Health Insurance Plan: Reducing Costs & Improving Quality
Health Care Reform Should Expand Consumer Choice • We should be able to keep our employer-provided coverage if we like it. • We should be able to get coverage through a new public health insurance plan like Medicare sponsored by the government. • President Obama’s reform plan proposed such a choice for many Americans, as do many members of Congress. • Medicare is a public health insurance plan for seniors that should continue and be improved. • Medicare provides valuable lessons for creating a newpublic health insurance plan for people under 65.
Public Health Insurance Plans: Strong Track Record vs. Private Insurance Plans • Much better cost controls • Much lower administrative costs • Much more reasonable provider costs • Good quality and cost effectiveness • More choice, competition and accountability
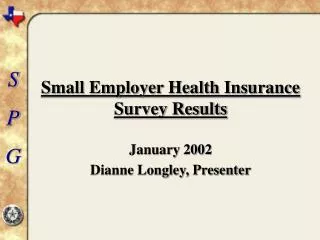
Medicare’s Record: Better Cost Controls than Private Insurance Over 25 Years • Private health insurers’ spending per enrollee grew 29% faster than Medicare spending between 1983 and 2006. • Private health insurers’ spending per enrollee grew 59% faster than Medicare spending between 1997 and 2006. • Spending was for comparable benefits. • The time periods correspond to major reforms to the way Medicare pays hospitals (1983) and physicians (1997).
Per Enrollee Average Annual Percent Change in Private Health Insurance Premiums and in Medicare Spending for Common Benefits 7.6% 8% 7.3% 7% 5.9% 6% PHI 4.6% 5% Medicare 4% Trend PHI 3% Trend Medicare 2% 1% 0% 1983-2006 1997-2006 Source: Centers for Medicare & Medicaid Services, Office of the Actuary, National Health Statistics Group, National Health Expenditures, Table 13, 2008
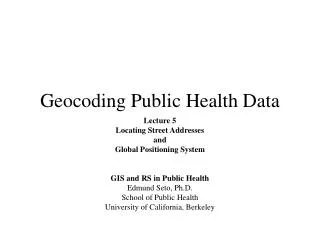
“Excess Spending Growth” for Elderly Health Care Is Much Lower than for the Non-elderly • Excess spending growth measures how much is spent on health care above how much the economy grows. The goal is not to spend more than the economy grows, or else health care becomes too costly. • Excess spending growth for the elderly, nearly all of whom get Medicare, has plummeted to just 0.3% in recent years. • Excess spending growth for the non-elderly, most of whom are privately insured, has skyrocketed to 3.4% -- that’s unaffordable. • Much lower spending for seniors is due to Medicare’s much stronger cost control measures.
Annual Rates of Excess Growth in Health Spending Per Person for Selected Time Periods, Elderly and Nonelderly, 1970–2004 5% Elderly 4% Nonelderly 3% 2% 1% 0% 1970-1977 1977-1987 1987-1996 1996-2004 Source: Chapin White, “Why Did Medicare Spending Growth Slow Down?” Health Affairs, May/June 2008.
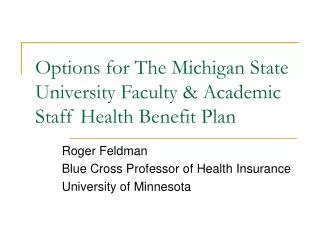
Medicare’s Record: Much Better Cost Controls Than Private FEHBP Plans • The Federal Employees Health Benefits Program offers members of Congress and other government employees a choice of hundreds of private insurance plans through an “insurance exchange.” • The annual growth in FEHBP plan premiums per enrollee was 26% higher than the growth in Medicare spending between 1985 and 2002 (latest data). • FEHBP plans’ costs rose at the same rate as other private health insurance plans. • FEHBP is not a good model for a national health insurance exchange.
Annual per Enrollee Growth in Medicare Spending and Private Health Insurance and FEHBP Plan Premiums For Common Benefits, 1985–2002 7.4% 7.3% 8% 7% 5.8% 6% 5% 4% 3% 2% 1% 0% Medicare PHI FEHBP Source: Katharine Levit et al., "Health Spending Rebound Continues In 2002,” Health Affairs, Jan/Feb 2004
Private Health Insurance Market: Highly Consolidated, High Premiums, Record Profits • In 16 states the dominant carrier has at least 50% of private insurance enrollment. • In 40 states the top 3 carriers have 60% to 100% of the market. • Employer-paid health insurance premiums have increased 9% a yearsince 1999. • The result: Insurance companies reap record profits. • The need: More competition from a public plan.
Market Consolidation: Record Insurance Company and Hospital Profits • Profits of the 14 largest health insurance companies rose from $3.5 billion to $15 billion between 2000 and 2007 – a 330% increase. • CEOs at these companies were paid a combined $147.6 million in 2007 – $10.5 million each. • That’s 259 times more than an average worker was paid -- $40,690. • 9 out of 10 metro areas are highly concentrated hospital markets pushing up costs in some markets by 40%. • U.S. for-profit hospitals reported $43 billion in profits in 2007, their best single-year jump in at least 15 years.
Growth in Profits of Major Private Health Insurance Companies $15.0 Billion $16 $14 $12 $10 $8 $6 $3.5 Billion $4 $2 $0 2000 2007 Source: Company SEC filings
Profits and CEO Compensation for Major Private Health Insurance Companies Source: Company SEC filings. The companies are listed in the Corporate Library's "Insurance Health and Disability" category. All of these companies, with the exception of Torchmark, are members of America's Health Insurance Plans. *Sierra Health Services has been acquired by UnitedHealth Group. **WellCare Health Plans did not exist in 2000 and it has not filed quarterly or annual reports since 2007 when its offices were raided by the FBI. Its CEO compensation figure is from 2006.
Public Health Insurance Plans = Much Lower Administrative Costs • Medicare’s public plan has administrative costs of less than 2%. • Administrative costs and profits of Medicare Advantage plans, offered by private insurers, are 11%. • Health insurance industry spending for administration and profits jumped 12% a year from 2000 to 2005: • 40% faster than overall health spending grew • 50% faster than hospitals’ and physicians’ spending grew • Private health insurance industry employment grew 52% from 1997 to 2007; private health plan enrollment of those under 65 grew by just 3.4%.
Health Expenditure Growth by Selected Categories, 2000-2005 14% 12.0% 12% 10.7% 10% 8.0% 7.9% 8% 6.1% 6% 4% 2% 0% Insurance Prescription Hospital Care Physician & Nursing Home & Administration & Drugs Clinical Services Home Health Profit Source: The Commonwealth Fund Commission on a High Performance Health System, "Slowing the Growth of U.S. Health Care Expenditures: What Are the Options?” January 2007
Growth in Employment, Aug. 1997- Aug. 2007 60% 52% 50% 40% 26% 30% 20% 12% 10% 0% Health Insurance Health & Support Total Nonfarm Industry Services Source: Economic Policy Institute chart based on Bureau of Labor Statistics, Employment Statistics Survey (National)
Public Health Insurance = More Bargaining Power and Lower Provider Costs • Hospitals:Paid25% less by Medicare than private insurers pay for comparable benefits. Virtually all hospitals participate with Medicare. • Medicare’s more reasonable hospital payments require them to operate more efficiently. • Physicians: Paid 19% less by Medicare than private insurers pay for comparable services. • 97% of doctorstake new Medicare public plan patients, virtually the same rate as accept private PPO patients. • Number of physicians billing Medicare is growing much faster than enrollment in Medicare Part B, which pays for physician care.
Public Health Insurance Plans = High Quality and Cost Effectiveness • Medicare’s central role: Health policy experts say Medicare plays the central role in transforming the health system to higher quality and more cost effectiveness. • Medicare is leading: Development of practice guidelines and quality measurements, requiring providers to publicly report quality indicators, development of a pay-for-performance system. • Market share: Medicare and a new public plan would have the market share and power to reshape market practices to promote much better quality and more cost effectiveness. • More financial incentives: Public health insurance plans have more incentive than private plans to improve quality in order to curb costs because they operate under tight fiscal constraints and can’t pass along cost increases to employers. • Stability: Public health insurance plans are much more stable for enrollees and providers making investments in prevention much more cost effective for the long run.
Public Health Insurance Plans = More Choice, Competition and Accountability • Choice: A public plan offers an alternative to private insurance and access to more health care providers. • Competition: Between public and private plans will place an important check on both plans to the benefit of consumers. • Accountability: A public plan promotes accountability because it must meet the test of democratic support. • Transparency: Private insurers’ billing, payment, claims and health outcomes data are mostly proprietary and receive limited public oversight.