Download
1 / 51
530 likes | 719 Vues
Gastric Bypass Patient Education. Treatment of Obesity. Obesity Classification. Obesity has reached epidemic proportions in the U.S. over the past 20 years¹. U.S. Pop. BMI. Classification. Overweight > 25.0 64 %

E N D
Obesity Classification Obesity has reached epidemic proportions in the U.S. over the past 20 years¹ U.S. Pop BMI Classification Overweight > 25.0 64 % Obese (Class I) 30.0 - 34.921 % Obese (Class II) 35.0 - 39.9 Clinically Severe Obesity (Class III) > 40.0 6 % 1 CDC: www.cdc.gov - accessed 2002 BMI: Body Mass Index = weight/(height)2 kg/m2
<10% 10%-14% 15%-19% 20% Obesity1 Trends Among U.S. Adults 1BMI > 30, or ~ 30 lbs. overweight for 5’4” person
Genetic Environmental Behavioral Multifactorial Disease
Osteoarthritis Hypertension GERD Urinary Stress Incontinence Gallbladder Disease Depression Diabetes Hyperinsulinemia Asthma Sleep Apnea Congestive Heart Failure Anemia Neoplasia Dyslipidemia Obesity is Associated with Significant Comorbidities
Comorbid Conditions • Almost 80% of obese adults have one of the following: • Diabetes • Dyslipidemia • Coronary Artery Disease, Hypertension • Gallbladder Disease • Osteoarthritis • Almost 40% have two or more of the above conditions
Obesity Increases Mortality “Taken together, the diseases associated with morbid obesity markedly reduce the odds of attaining an average life span and raise annual mortality tenfold or more.” American College of Surgeons, Recommendations for facilities performing bariatric surgery, ST-34, Bull Am Col Surg, 2000;85:
Non-Surgical Treatment • Medication • Diet and exercise • Behavior modification • Weight loss is not substantial for 90 – 95 % of patients with clinically severe obesity using these methods. • Weight is usually regained within five years.
Medical Treatment of Obesity Medical Complications of Pharmacotherapy
Why Surgery for the Treatment of the Clinically Severe Obese? • “Only surgery has proven effective over the long term for most patients with clinically severe obesity.” NIH Consensus Conference Statement, 1991 • Surgery for the treatment of clinically severe obesity is endorsed by: The National Institutes of Health The American Medical Association The National Institute of Diabetes and Digestive and Kidney Diseases American Association of Family Practitioners
Who is Eligible for Bariatric Surgery? The NIH Consensus Panel recommends that: • Patients have a Body Mass Index > 40 kg/m2 • 100 lbs. or more overweight • Patients have a Body Mass Index between 35 and 40 kg/m2 with significant comorbidities • Patients have failed other medically managed weight-loss programs 6% of the U.S. Adult Population(Over 10 Million People)Meet These Criteria
Ineligible patients Exclusion Criteria: • Obesity related to a metabolic or endocrine disorder • History of substance abuse or untreated major psychiatric disease • Surgery contraindicated or high risk • Women who want to become pregnant within the next 18 months
Review of the Digestive System • Esophagus • Stomach • Small Intestine (Duodenum, Jejunum, Ileum) • Large Intestine
Malabsorptive Restrictive Combination Adjustable Band Gastroplasty Biliopancreatic Diversion w/ Duodenal Switch Roux en Y Gastric Bypass Bariatric Surgery Today Three Types of Most Commonly Performed Bariatric Surgery Procedures
Relatively easy surgical procedure Less dietary deficiencies Less weight loss More late failures due to dilation Less effective with sweet eaters Significant dietary compliance Restrictive Surgery Adjustable Band Gastroplasty
Greater sustained weight loss with less dietary compliance Increased risk of malnutrition and vitamin deficiency Constant follow–up to monitor increased risk Intermittent diarrhea Malabsorptive Surgery Biliopancreatic Diversion w/ Duodenal Switch
Long term sustained weight loss No protein-calorie malabsorption Little vitamin or mineral deficiencies Technically difficult procedure Roux-en-Y Gastric-Bypass Roux en Y Gastric Bypass
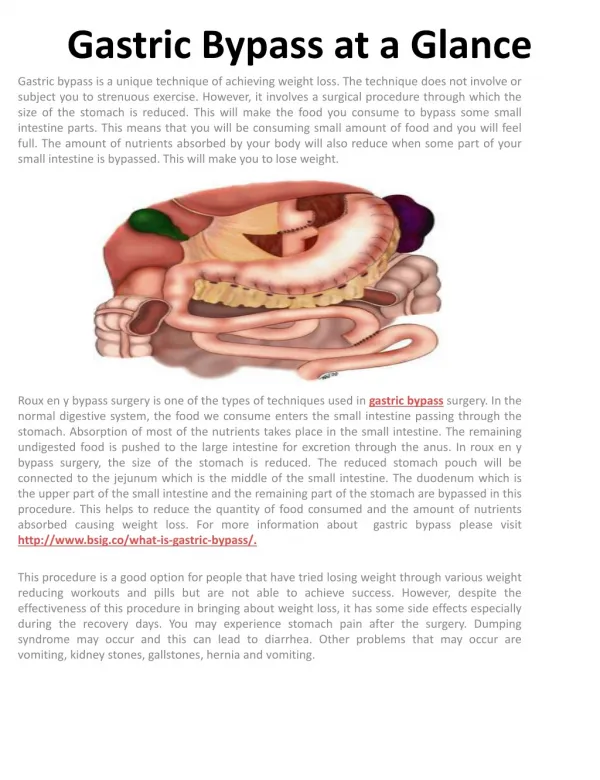
The Roux-en-Y Gastric Bypass 1. A small, 15 to 20 cc, pouch is created at the top of the stomach. 2. The small bowel is divided. The biliopancreatic limb is reattached to the small bowel. 3. The other end is connected to the pouch, creating the Roux limb. The small pouch releases food slowly, causing a sensation of fullness with very little food. The biliopancreatic limb preserves the action of the digestive tract.
Open Increased post op pain, longer hospitalizations Increased incidence of wound complications - infections, hernias, seromas Return to work in 4-8 weeks Laparoscopic Less post op pain, early mobility Wound complications may be significantly reduced 2-3 day hospital stay Return to work in 1-3 weeks Evolution of Laparoscopic Technique in Bariatric Surgery
Sustained Weight Loss % Excess Weight Loss as a function of time Pories et al. Ann Surg 1998 May;227(5):637-43; discussion 643-4 Schauer et al Ann Surg 2000 Oct;232(4):515-29 Wittgrove et al Obes Surg 2000 Jun;10(3):233-9
Bariatric Surgery as a Tool Bariatric surgery will not work alone. Commitment to diet, exercise and support are intricate parts of your weight loss success.
47 41 47 41 33 63 33 63 24 72 24 72 18 70 18 70 19 74 19 74 29 57 29 57 55 41 55 41 39 44 39 44 69 13 69 13 18 82 18 82 35.1% 55.7% 35.1% 55.7% 90.8% 90.8% Improved or Resolved Improved or Resolved Resolution of Comorbidities Number N= 104 Prior to % % No - % % 1 year post-op Surgery Worse Change Improved Resolved Osteoarthritis 64 2 10 Hypercholesterimia 62 0 4 GERD 58 0 4 Hypertension 57 0 12 Sleep Apnea 44 2 5 Hypertriglyceridemia 43 0 14 Peripheral Edema 31 0 4 Stress Incontinence 18 6 11 Asthma 18 6 12 Diabetes 18 0 0 Average 1.6% 7.6% Schauer, et al, Ann Surg 2000 Oct;232(4):515-29
Open and Laparosopic Roux-en-YBypass Complication Rates Meta Analysis Lap Open Mortality < 1.5 % < 1.5 % Leak Rate < 3.1 % < 3.0 % PE Rate < 0.6 % < 1.5 % Hernia Rate 6.6 - 18 % < 1.8% Wound Infection Rate 5 - 18% < 2% Schauer and Ikramuddin, Surg Clin North Am, 2001 Oct;81(5):1145-79 Kral, Clin Per Gastroenterology 2001 Sep/Oct:295-305 Nguyen et al. Ann Surg, 2001;234(3)279-291
Possible Complications (may lead to short or long term hospitalization and/or re-operation) • Infection, bleeding or leaking at suture/staple lines • Blockage of the intestines or pouch • Dehydration • Blood clots in legs or lungs • Vitamin and mineral deficiency • Protein malnutrition • Incisional hernia • Death
Possible Side Effects • Nausea and vomiting • Gas and bloating • Dumping syndrome • Lactose intolerance • Temporary hair thinning • Depression and psychological distress • Changes in bowel habits such as diarrhea, constipation, gas and/or foul smelling stool
Post-Operative Summary On average, Gastric-bypass patients . . . • Will find that they have lost 65- 80% of their excess body weight, the majority of it in the first 18 to 24 months after surgery. • May have rapid improvements in the morbid side effects of their obesity, such as type 2 diabetes, high blood pressure, sleep apnea, and high cholesterol levels.
Pathway to Bariatric Surgery • Patient Responsibilities • Honesty, Responsibility, Cooperation • Bariatric Program Responsibilities • Honesty, Responsibility, Cooperation
Initial Contact Pre-Op Information Exchange Preoperative Evaluation Surgery Post-Op Follow-up and Support What will your care pathway look like?
Who is my dedicated team ? • Surgeon • Registered Nurse Coordinator • Registered Dietitian • Psychologist / Social Worker • Exercise Specialist • Insurance Coordinator • Administrative Assistant
What Medical Specialists are Involved? • Gynecology • Gastroenterology • Anesthesiology • Reconstructive Surgery • Pulmonology • Internal Medicine • Cardiology • Endocrinology Multidisciplinary Approach
Support groups – the heart of the program • Create fellowship through a common bond • Provide a source of up-to-date information about surgery and latest developments • Educate in nutrition, exercise, and post-op needs • Promote networking • Increase bariatric surgery success • Support life-style changes
Pre-operative Diet Goals Begin creating healthy nutritional patterns: • Multivitamin and mineral intake • Adequate fluid intake • Quality versus quantity • Avoiding the last supper syndrome
Diet • Stage I: A low sugar, clear liquid diet, started two to three days after surgery. It essentially provides hydration during the initial post-operative phase.
Diet (cont.) • Stage II: A full liquid diet providing all the essential requirements for the first post-operative month. Patients go home from the hospital on the stage II diet. • Stage III: A modified solid diet. The surgeon instructs the patient when to advance to this diet. Introducing semi-solid food or solid diet too early may lead to obstruction and vomiting. It may also unduly stress the anastomosis.
Foods that may be difficult to tolerate • Bread products • Cow milk products • Pasta products • Fatty foods and fried foods • Candy, chocolate, any sugary foods and beverages • Bran cereal and other bran products • Corn, whole beans, and peas • Dried fruits and skins of fresh fruit • Coconut • Carbonated beverages
Fluids • Recommended fluid intake: min. 2 Liters/day • Non-carbonated • Non-calorie • Not during meals • Continually sip water throughout the day to ensure adequate hydration • Avoid caffeinated beverages • Avoid straws
Vitamins, Minerals and Supplements • Liquid protein supplements required to reach 75 grams of protein per day • Multivitamin with Iron morning and evening • 1000 mg of folate/day • B-12 supplementations • 500 mg of Calcium Citrate three times per day • Other supplements on an individual need basis • Periodic blood levels must be taken to ensure adequate nutrition
Dumping Syndrome Dumping Syndrome • Early: immediately associated with food intake (GI symptoms) • Late: delayed onset, usually 1 ½ to 2 hours after food intake (neurological symptoms) • Some patients never experience Dumping Syndrome Some surgeons consider dumping syndrome to be a beneficial effect of Gastric Bypass surgery. It provides a quick and reliable negative feedback for intake in the “wrong” foods.
Long-term Diet Goals • Avoid concentrated sweets due to high calorie content and the possibility of dumping • Low fat, heart healthy diet • Maintain adequate water intake
Your Role Before Surgery • Commit to improving your health (diet, exercise, mental readiness) • Discuss your health history with your surgeon • Ask questions and vocalize concerns that you may have about surgery or your care • Commit to following all instructions on nutrition, activity and other care after surgery
Your Commitment • Adhere to diet • Exercise daily • Commit to lifelong follow-up • Attend at least 2 support group meetings pre-op and participate regularly post-op. • Buy and take in vitamin and mineral supplements for the rest of your life • Avoid tobacco products lifelong and alcohol for at least 1 year post-op.