Download

1 / 30
300 likes | 314 Vues
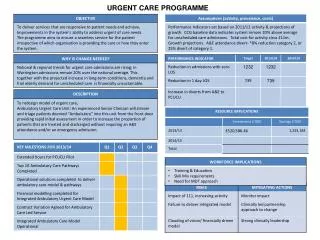
This report examines the different aspects of urgent care delivery and provides insights on how to improve and measure the quality outcomes. It includes findings and recommendations for general practice, A&E, and acute services. A web-based planning and monitoring tool is being developed to help practices benchmark their performance and make evidence-based changes. The report also highlights the importance of effective commissioning and monitoring of out-of-hours services.

E N D
Measurement of Quality OutcomesMaking Sure Your Urgent Care Delivers April 2011 David Carson 07703 025775 david.carson@primarycarefoundation.co.uk
The Primary Care Foundation has looked urgent care from a number of angles Reports for Department of Health • Primary Care in A&E • Urgent Care in general practice • Benchmark of out of hours services • Urgent care centres (report with DH) Various projects for: • Hospital Trusts • PCTs • PBC Groups • Commercial and mutual provider organisations
A whole system perspective:urgent & emergency care components Patient • NHS Direct • General Practice • Out of Hours • Ambulance service • UCCS and WICs • Community Services • A & E From any of the above From clinicians Self care Episode complete Hospital Obs & Gyn Ortho Surgery Acute medicine Each component must work well - separately and as part of the whole
Topics that I aim to cover... • General Practice In and Out of Hours • A&E • Acute Services
Some of our key findings • Speed of initial response – or ensuring patients can get through - matters • Review and understand your number of appointments and the proportion that can be booked same day • Managing peaks in demand - such as Monday mornings – is important • Practice staff need to recognise what is potentially urgent and agree how to respond • Rapid clinical assessment is important – especially of requests for home visits • Telephone consultation can play a useful role
Acute Admission Timeline 2 (often 4) Hours 3 Hours 2 Hours 17.30 13.30 8.30 11.30 Just as hospital staff go home! 1 Hour 15 Minutes 1 Hour 10.45 09.45 8.30 8.45 In time to set up alternative to hospital Early enough to avoid risk of deterioration
A new approach • Currently developing a web based planning and monitoring tool. Focuses on: • Telephony – checking the capability to answer the phone promptly • Capacity in terms of appointments to meet the demand from patients • Recognition of potentially urgent cases • Response to urgent cases • Brings together practice data and patient experience to give a strong evidence base for making changes • Practices are able to benchmark their own system and process against other local practices and across England
Better evidence supporting change • Range of indicators provide a rounded picture of what is happening in the practice, including: • staffing by hour answering phones compared to what is needed for an effective response (Erlang Formula) • consultation rate, weighted for age, compared to national average • Detailed report builds on how the practice understands its processes with analysis of data and options for change • Tweaking process will not work if people can’t get through on the phones or there are too few appointments • Once these issues are addressed, there are a range of options – the practice will need to identify what works for them
Outcome of intervention • Cons rate of 10 last July • Could not get through on phone • Difficult to see doctor of choice • January • Cons rate 6 • Less pressure • Continuity improved • Quality improved
The CQC investigation highlighted shortcomings in commissioning • Out-of-hours services were low priority at the time and the PCTs had limited understanding of these services. • There was a lack of leadership in commissioning and monitoring services as part of an integrated urgent care service. • There was a lack of experience in the PCTs in contracting with a commercial organisation. • Staff did not fully understand the national quality requirements or TCN’s reports on activity and performance • The PCTs did not have a high standard of commissioning or contract monitoring in out-of-hours - these contracts should have been monitored more thoroughly. • Not highlighted in national targets and finances – so not seen as a priority for SHAs or PCTs.
The Health secretary believes that GP Commissioners will fix it!
Key message – you get what you insist onAlternatively, you get what you deserve • You need a wide range of measures – and making comparison is vital • Services have to manage clinicians if they are to perform effectively and consistently • Each part must work well if you are to have a hope of joining different parts – and a similar wide range of measures is needed • You will need to look at how practices deliver their share of care • Look to establish contracts for longer and to drive improvements over a period
What qualities should data about a clinical service exhibit? • Competently collected and collated • Correct • Clear, well presented information • Consistent – to allow comparison within the data set and over time • Complete – it should provide a full picture of all aspects • Compare and contrast outcomes – so we can understand the cause of differences and which innovations work • Collaborative - to secure the information and to engage stakeholders • Communicate – so that users can understand what it means • Convincing – if users are to change what they do based on the evidence • Challenge or corroborate assumptions about clinical practice and outcomes • Costed – because of the requirement for efficiency we need this too
A wide range of measures to give a rounded picture is needed if perverse incentives are to be avoided Out of Hours benchmark • % definitively assessed in 20 and 60 minutes • % answered in 60 seconds • % with face to face consultation in 1, 2 and 6 hours • % of urgent cases • Patient experience • % of patients going to 999/hospital • Cost per case, cost per head • Productivity
There are big differences between services delivering out of hours care (this looks at QR9 for urgent cases in 20 minutes….)
..and there are big differences in what they identify as urgent Those with higher levels of urgent on receipt find it difficult to better 90% definitively assessed in 20 minutes These have low %urgent on receipt but have a low percentage of urgent cases assessed in 20 minutes
In general it costs more to provide OOH cover in a rural PCT than an urban one (but there are wide variations within any band)
There is a clear relationship between IPSOS Mori respondent’s view of speed of response and the rating for the care received
The majority of services give telephone advice in 40 to 50% of cases and offer home visits to 10 to 17%. % Advice % Home visits
A&E Proposed Measures • Ambulatory care • Unplanned re-attendance • Total time spent • % leaving before being seen • Patient experience • Time to initial assessment • Time to treatment • % with consultant sign-off
There are big differences between services (four A&E departments looking at % discharged by 10 minute slots) 28.5% admitted 19.6% admitted 22.7% admitted 18.3% admitted 13.9% admitted 30.7% admitted
What do people often focus on? • Numbers of attendances • Admission avoidance • Quality = Volumes (or lack of them) • What about people who need hospital
Process integrated and not competativeGPs are part of the process – Not in front of it
Acute care • Ambulatory sensitive conditions – Outcomes • Percentage discharged same day • Process and timely care – Rapid Care is often good care • Readmission rates • Time to theatre for # NOF • Stroke – compliance with pathway • Etc etc
So what have we been missing? • Professionals and organisations have been competing • GPs - we manage risk better than A&E • A&E - We deliver detailed and proper assessment • Etcetc • Each group has specific and valuable expertise • Build a system in which the expertise is complementary and cooperative and not competitive • I have never ever met a clinician who was admitting a patient because the trust would get a tariff payment!