Immunity
Immunity . Trisha Economidis, MS, ARNP Spring, 2014. WAR DECLARED…. We are at war with our environment Troops are prepared to fight from every sector of the body to keep us safe (and healthy) Regiments on the ready include: Antibodies Immunoglobulins White Blood cells


Immunity
E N D
Presentation Transcript
Immunity Trisha Economidis, MS, ARNP Spring, 2014
WAR DECLARED….. • We are at war with our environment • Troops are prepared to fight from every sector of the body to keep us safe (and healthy) • Regiments on the ready include: • Antibodies • Immunoglobulins • White Blood cells • Immune Response Teams: Antibody-mediated and Cell-Mediated Immunity • And others…….
Immune System Review: Public Enemy Number ONE • Antigen – a protein that stimulates an immune reaction, causing production of antibodies. • Viruses • Bacteria • Fungi • Parasites • Etc…..
Immune System Review • Antibody – a globulin (PRO) produced by B cells as a defense mechanism against foreign materials. Combines in a lock and key style with antigens
Meet the Troops: WBC’s – Name, Rank & Serial Number • Reported in a CBC as WBC Count and Differential • Granulocytes (basophils, eosinophils, neutrophils – BEN) • Basophils – 0.5 – 1% of total WBC’s. Release histamineand heparin granules – increase in hypersensitivity reactions • Eosinophils– 1-4% - Destroy helminths, mediate allergic reaction • Neutrophils – 55-70%. First to arrive – Phagocytize! • Bands – Immature neutrophils (5% of total WBCs) • Segmented (Segs) – Mature neutrophils (55% of total WBCs)
WBC’s, continued • Monocytes – 2-3% Phagocytize directly • Lymphocytes – 20-40% • T lymphs – recognize, attack and destroy antigens • B lymphs – produce immunoglobulins to attack and destroy antigens • NK (Natural Killer) cells – kill foreign pathogens
First Line of Defense:Innate Immune Response • Soldiers of the Innate Immune Response: • Neutrophils • Macrophages • NK cells Defenses Provided: • Barrier Protection • Inflammation • Phagocytosis GOAL: Neutralize and Destroy the Invaders
Innate Immune Response:Barrier Protection • Prevents organisms from entering the body • Skin • Respiratory Tree • Tears/Saliva • GI Tract – acidic environment, peristalsis • Bile – antimicrobial • GU tract – mucous membranes
Innate Immune Response: Inflammation • Begins when histamine and other chemical mediators of inflammation are released directly from damaged cells Histamine/chemical release Dilation and increased Permeability of blood vessels flow of phagocytes, antimicrobials, O2, & nutrients to area of damage
Innate Immune Response: Phagocytosis • Phagocytosis • PHAGOCYTES TO THE RESCUE!
Second Line of Defense: Adaptive Immune Response • Body recognizes and destroys pathogens encountered before • Demonstrates self-recognition • Specific – stimulated by and directed toward specific antigens • Generalized, systemic – not limited to site of injury • Has a memory – repeated exposures to antigens produce a more rapid response
Adaptive Immune Response • Cell Soldiers: Lymphocytes – WBCs that mature to either T cells or B cells
Adaptive Immune Response: Military Forces • Antibody-Mediated Immune Response • Cell-Mediated Immune Response
Adaptive Immune Response:Antibody-Mediated Immune Response • B cell Defense: • Activated by contact with an antigen • Proliferate and morph into • 1. Plasma cells (producing immunoglobulinsthat will bind to and destroy antigens) • 2. Memory cells – store the antibody-producing information for future encounters
Immunoglobulins (Ig) – the Special Agents of Antibody-Mediated Immune Response • IgM – Goes after “first time offenders” • IgG – most common one. (AKA: Gamma Globulin) – Active against bacteria and viruses
Immunoglobulins, cont. • IgE – primarily responsible for allergic response and parasitic infections • IgA – secreted by mucous membranes around body openings. Provides more protection for points of entry. • IgD – found of surface of B cells. Trap potential pathogens
Adaptive Immune Response:Cell-Mediated Immune Response • T cell Defense: Acts to destroy body cells that have become infected • Cytotoxic (Killer) T cells • Helper T cells • Suppressor T cells • Memory T cells
The nurse is caring for a client who has suffered an injury in which the skin is broken. In what order does the nurse anticipate assessing the occurrence of the following pathophysiological responses? Place the options in order.
1. Breach in the barrier of defense • 2. Vasodilation of the arterioles and venules • 3. Phagocytosis • 4. Margination and emigration of leukocytes into the damaged tissue • 5. Reconstruction
Correct Answer: 1, 2, 4, 3, 5 • Breach in the barrier of defense • Vasodilation of the arterioles and venules • Margination and emigration of leukocytes into the damaged tissue • Phagocytosis • Reconstruction
Immunity Terms: • Immunocompetent – immune system capable of responding to pathogens and mounting an immune response • Immunocompromised – immune system is incapable of normal reaction to pathogens as result of a disease • Immunosenescence – age-associated decline of the immune system • Immunosuppression – Prevention of an immune response with drugs
Which of the following atypical findings would the nurse look for in an older adult client who presents with an infection? • A. Fever and chills • B. Erythema and edema • C. Behavioral changes and confusion • D. Leukocytosis with elevated neutrophil count
Correct Answer: C • Mental status changes ranging from restlessness to confusion comprise one of the most frequent “atypical” signs of infection in older adults.
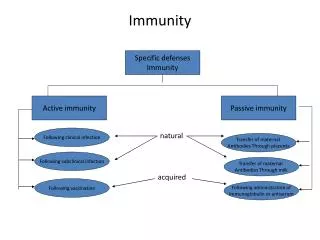
Types of Immunity • Active Immunity – occurs when the body produces antibodies or develops immune lymphocytes against specific antigens • Naturally acquired – occurs when we have a disease, the body produces antibodies, and the risk of having the disease again is very low. • Artificially acquired – occurs with vaccination; immune system is stimulated with the killed or attenuated organism, produces antibodies and memory cells, but not the disease
Types of Immunity • Passive Immunity – Provides temporary protection against disease-producing antigens when we receive antibodies produced by other people or animals • Naturally acquired – occurs with maternal transfer of antibodies via the placenta and breast milk • Artificially acquired – occurs with administration of antibodies or antitoxins in immune globulin; i.e. Rabies human immune globulin
When a patient receives gamma globulin following exposure to hepatitis A, the nurse expects the patient to develop which of the following? • A. Natural passive immunity • B. Natural active immunity • C. Acquired passive immunity • D. Acquired active immunity
Correct Answer: C • Acquired passive immunity is the result of a gamma globulin infusion following exposure to hepatitis A. This type of immunity is short-lived and usually lasts only about 4 weeks.
A client receives a polio vaccine during a clinic visit. The nurse explains that this will provide what type of immunity to the client? • A. Active naturally acquired immunity • B. Active artificially acquired immunity • C. Passive naturally acquired immunity • D. Passive artificially acquired immunity
Correct Answer: B • Active artificially acquired immunity
Assessment of the Immune system • Chief complaint – subjective data • Review biographic data: age, gender, race, ethnic background, family history • Comprehensive health history • Physical Assessment
Immune System Diagnostics • WBC with differential (refer to slide 5 for specifics on the differential, and to chart on page 288 in LeMone)
Shift to the Left?????? • In an acute infection more lymphocytes are produced • A “shift to the left” occurs when there are more bands (immature or baby neutrophils) in circulation than there are segs (mature or grownup neutrophils) (more bands than segs in circulation) Larger number of cells”shift to the left” on the maturation chain.
“Shift to the left” • Higher number of bands than segs (usually when bands reach 6%) in circulation called bandemia. • Indicates body is responding to an acute infection, usually bacterial, or to Stress (i.e. women in childbirth)
The patient with an acute infection shows a shift to the left on the WBC differential count. The nurse recognizes a shift to the left because of which laboratory finding? • A. Increased band neutrophils • B. Increased eosinophils • C. Decreased leukocytes • D. Decreased monocytes
Correct Answer: A • Increased band neutrophils is a response to bacterial infection. This is called a “shift to the left.”
Immune System Diagnostics • ELISA/Western Blot • HIV rapid antibody test • CD4-T cell counts (Helper T’s) – reflection of immune status (normal: 500-1600 cells/mm3) • HIV Viral Load testing – measures the presence of HIV viral genetic material in the patient’s blood rather than the body’s response to the virus
Immune System Diagnostics • Antibody Testing • ANA (Antinuclear Antibody) • Rheumatoid Factor • Complement Assay • ESR (erythrocyte sedimentation rate) – SedRate – Values: Female: 1-20 mm in 1 hr; Male: 1-15 mm in 1 hr • HLA testing – Human Leukocyte Antigen • Lupus erythematosus cell test • Anti CCP antibody test
Health Promotion and the Immune System – Boosting your Immunity • Diet – Balanced diet • Exercise – Regular, moderate work-outs • Stress relief • Get enough sleep • Use sun exposure protection • Quit smoking or Don’t Start • Avoid excess alcohol • Immunizations up-to-date
Pharmacologic Management of Immune Disorders • Antibiotics (anti-infectives) • Use: treatment/prophylaxis of bacterial infections • Cautions: Can depress bone marrow; Allergies; Organ Toxicity; Superinfections • Penicillins Macrolides • Cephalosporins Aminoglycosides • CarbapenemsOxazolidinones • VancomycinFluoroquinolones • Tetracyclines Sulfonamides • Flagyl
Pharmacological Interventions • Antivirals – Destroy viruses either directly or by inhibiting the ability to replicate • acyclovir (Zovirax); HSV-1, HSV-2, VZV • Amantadine - prevention and tx of Type A influenza; vosetamivir (Tamiflu), Influenza Types A & B
Pharmacological Interventions • Antifungals • Kill or stop growth of fungal infections of skin, mucus membranes, as well as systemically • Topical • Clotrimazole, ketoconazole, miconazole, nystatin • Systemic • Amphotericin B, fluconazole, ketoconazole
Pharmacological Interventions • Antihistamines • Relief of symptoms associated with allergies, rhinitis, urticaria • 1st generation-sedating • Chlor-trimeton (chlorpheninamine) • Dramamine (dimenthydrinate) • Benadryl (dephenhydramine) • Atarax, Vistaril (hydroxyzine) • 2ndgeneration-non-sedating or less sedating • Allegra (fexofenadine) • Claritin (loratadine) • Zyrtec (cetirizine)
Pharmacological Interventions • Corticosteroids • Used for anti-inflammatory and immunosuppressive properties • Topical, inhaled, intranasal, ophthalmic, IV, PO, IM • Long, intermediate, and short-acting
Pharmacological Interventions • Adrenergic sympathomimetic - Epinephrine • Inhibits release of hypersensitivity mediators • Inhibits reaction from mast cells • Produces bronchodilation, vasoconstriction • Epinephrine (Adrenalin) • 0.3mg-0.5 mg of 1:1000 subcutaneously or IM (Adults)
Pharmacological Interventions • Immunotherapy • SC injections weekly/biweekly of allergen extracts • Goals of Therapy • Stimulate IgG levels for allergen binding • Decrease IgE levels • ALWAYS EXPECT ADVERSE REACTIONS!!!