Download
1 / 40
410 likes | 1.27k Vues
Neonatal Surgical Issues (Part 1). Sue Ann Smith, MD Neonatologist. An anatomic survey. Head and Neck lesions Chest lesions Abdomen Abdominal wall defects and infection. The Nose. Choanal atresia – bilateral atresia Respiratory distress resolves with crying

E N D
Neonatal Surgical Issues(Part 1) Sue Ann Smith, MD Neonatologist
An anatomic survey • Head and Neck lesions • Chest lesions • Abdomen • Abdominal wall defects and infection
The Nose • Choanal atresia – bilateral atresia • Respiratory distress resolves with crying • Treat with oral airway until surgical repair • CT scan often used in surgical planning • ENT surgeons make opening in bony plate and stent open during healing • Nasolacrimal duct cysts – large and bilat • Respiratory distress resolves with crying • Treat with oral airway • Can usually be seen with otoscope
Robin sequence • AKA Pierre Robin syndrome • Hypoplastic mandible with U-shaped midline cleft palate • Respiratory and feeding difficulties • Position prone, may require nasopharyngeal tube, oral airway, LMA, or endotracheal tube • Mandibular distraction is now treatment of choice at OHSU
The Unusual • Laryngotracheal clefts • Laryngeal webs • Tracheal agenesis – frequently lethal • Neck masses • Foregut duplication cyst • lymphangioma
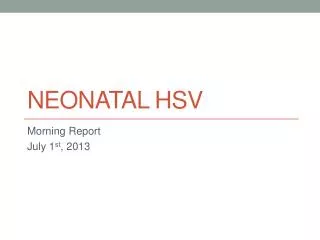
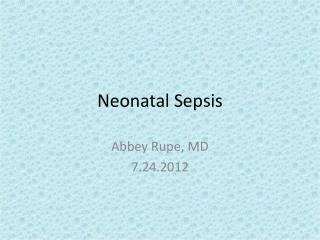
Normal Larynx Laryngeal Web
Congenital Chest Lesions • Tracheo-esophageal fistula • Diaphragmatic Hernia (briefly) • Congenital lobar emphysema • Cystic adenomatoid malformation • Vascular rings
Tracheo-Esophageal Fistula (TEF) • Esophageal atresia with TEF is most common (85%). • Diagnosis may be suspected antenatal with absence of stomach bubble and polyhydramnios. (*Caution: also seen with conditions that lead to poor swallowing) • Often associated with other anomalies: VATER and chromosomal
Tracheo-Esophageal Fistula (TEF) (cont) • Presentation: excessive salivation and intolerance of feedings. • Diagnosis: inability to pass catheter into stomach. • Pre-op Management: avoid mechanical ventilation (if possible), catheter to suction in the esophageal pouch, elevate head of bed.
Operative management • Ligation of fistula at trachea. • Mobilization of distal esophageal segment with primary anastamosis to proximal pouch. • NG tube left in place to stent open anastamosis while healing. • Chest tube left in for serous drainage usually.
Post-operative Management • Careful airway management to prevent trauma to the fistula ligation site in the trachea. • Prior to feedings, must make sure that the esophageal anastamosis does not leak. (swallow study) • Often have on going feeding problems. May need dilation procedures periodically
Other “TEFs” • Esophageal atresia without TEF – very rare • H-Type TEF-also rare. • Diagnosis usually after the neonatal period with frequent pneumonias or respiratory distress related to feedings
Congenital Diaphragmatic Hernia (CDH) • Most commonly on left side • Incidence 1:2000 to 1:5000 • Often associated with other malformations • Frequently diagnosed prenatally • Avoid bag-mask PPV
Pre-op CDH • Delayed surgical repair – usually after 72 hrs of age • NG drainage tube to keep bowel decompressed • Treat aggressively for pulmonary hypoplasia and Persistent Pulmonary Hypertension – including ECMO(?). • Surfactant therapy is now controversial
Post-Op CDH • “Anatomy is destiny” • Survival continues to be around 40-50%. • Feeding difficulties
Congenital lobar emphysema • Lesions that cause air trapping, with compression of surrounding tissue • Most common in left upper, right middle and right upper lobes • Usually attempt low volume ventilation. Sometimes selective intubation of other bronchus • May require surgical resection
Congenital Cystic Adenomatoid Malformation (CCAM) • May be confused with CDH • Abnormal lung tissue that forms fluid filled cysts. May be large cysts, or many small cysts and solid areas • Space occupying lesion • May cause shifting of mediastium • May spontaneously regress in fetus • May require surgical removal
Vascular Rings • Uncommon • Signs include stridor, vomiting and difficulty swallowing. • Barium swallow can be diagnostic, but may need chest MRI. • Sometimes may need cardiac catheterization
The Abdomen • Abdominal wall • defects • infection • Bowel • Obstructions
Gastroschisis • Abdominal wall defect to right of umbilicus with no covering over intestines • Rarely associated with other anomalies • Most babies are SGA and born to young mothers (why?) • 10% will have intestinal atresias • Rarely will have significant infarction of most of small bowel (i.e. lethal) • Most will have “meconium” stained amniotic fluid (really bile)
Gastroschisis Pre-op • Empty stomach (usually lots of bilious fluid) • NG tube for decompression • Place in bowel bag or wrap in warm saline soaked gauze and saran wrap • Support the bowel so as to maintain perfusion
Gastroschisis (post-op) • Primary closure is attempted • May require silo with slow return of intestine into small abdominal cavity • Maintain perfusion • Feeding difficulties are main post-op problem • At risk for adhesions throughout life
Omphalocele • Abdominal wall defect at umbilicus with covering (sac may rupture) • Frequently associated with other anomalies • Giant omphaloceles: respiratory issues with misshaped chest and airway malacias
Omphalocele • Decompress stomach initially • Careful eval for other anomalies • Intact sac may defer operation for years • “paint” membrane with betadine to toughen into a “rind” • Ruptured sac – repair similar to gastroschisis
Omphalitis • Presentation – erythema/induration of the periumbilical area with purulent discharge from umbilical stump. • Can spread extensively to abdominal wall or develop necrotizing fasciitis. • Both gram + and gram neg bacteria implicated • Full sepsis evaluation • Oxacillin/nafcillin and gent
Normal Larynx (upside down) Laryngeal Web (also upside down)