Download
1 / 19
190 likes | 268 Vues
Rare disorder causing cartilage inflammation. Airway involvement common and leads to high fatality. Case study of male farmer with cough and chest pain, diagnosed through histology and imaging.

E N D
Respiratory Tract Involvement in Relapsing Polychondritis(RP) Muthunayake M.T., Dassanayake D.L.B., Gamage L.N.Teaching Hospital, Kandy, Sri Lanka Introduction RP is a rare multisystem disorder characterized by inflammation of the cartilaginous structures of the body. Airway involvement is 50% and, is the major cause of death related to RP. 50% of deaths due to RP are due to respiratory involvement( 3,4). Male: Female -1:1. Average age at presentation: 47 years. History and Examination A 40 y old male farmer, Cough and pleuritic chest pain for 02 weeks, Fever for 04 days , No haemoptysis, wheeze, loss of appetite or loss of weight Clinical examination : unremarkable Investigations FBC: leukocytosis -15000mm-3 ESR: 123/1st hr 145/1st hr CXR : normal Sputum for acid fast bacilli : negative Mantoux : non-reactive Renal & liver functions : normal Blood picture : unremarkable ANA & rheumatoid factor : negative Rx started as lower respiratory tact infection 02 weeks later Developed pain in throat, nose, ears and, chest . Examination : tenderness of ears, nose, anterior neck and costochondral junctions Lung function tests : obstructive lung defect Histology* Auricular cartilage biopsy : Mixed inflammatory infiltrates, loss of normal basophilia, chondrocytes and destruction of lacunar architecture. Features are consistent with RP. Discussion MD-CT including HRCT of the chest is capable of demonstrating airway involvement in RP (1). Diffuse and smooth thickening of antero-lateral wall of the trachea with relative sparing of the posterior membranous wall is virtually pathognomonic of pulmonary involvement in RP (2). Tracheo-bronchial involvement is ideally demonstrated in mediastinal window. Lung algorithm is mandatory to visualize peribronchial thickening, focal air trapping and patchy atalectasis(2).These features were well appreciated in this case too. The most common CT finding of lower respiratory tract involvement in RP is increased airway wall attenuation (100%). Progressive cartilage calcification is a frequently reported feature of RP(6) and the degree of attenuation ranges from subtle to frank calcification. In our case no cartilage calcification was found but higher attenuation of airway wall was noted. As in our case, air trapping on expiration is well described key feature of RP and expiratory HRCT of chest is considered to be mandatory. (1) (2) (4) (3) Figure 1. Photograph of the of the right ear, inflamed (reddened) pinna Figure 2.Histology of auricular cartilage* Figure 3. Expiratory HRCT of the chest, diffuse peribronchial inflammatory infiltrates and air trapping (black arrow). Figure 4.CT thorax; diffuse, smooth thickening of antero- lateral tracheal wall. References 1. McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine 1976;55:193–215 2. Trentham DE, Le CH. Relapsing polychondritis. Ann Intern Med 1998;129:114–122Keren S. Lee, MD, Armin Ernst, MD, David E. Trentham, MD, Relapsing Polychondritis: Prevalence of Expiratory CT Airway Involvement, Radiology RSNA 2006, Aug; 240; 565-571. 3. Gergely P., Poor G. , Relapsing Polychodritis, Pract Best Clin 2004;18:723-738. 4. Armin Ernst, SamaanRafique, Phillip Boiselle., Relapsing Polychondritis ,CHEST2009; 135: 1024-1030. • 5. Tillie-Leblond I, Wallaert B, Leblond D, et al. Respiratory involvement in relapsing olpychondritis: • clinical, functional, endoscopic, and radiographic evaluations. Medicine1998;77:168–176 6. Jeffrey V. Behar ,Yo-Won Choi, et al. Relapsing Polychondritis Affecting the Lower Respiratory Tract, AJR:, January 2002;178:173-177.
Respiratory Tract Involvement in Relapsing Polychondritis(RP) MUTHUNAYAKE M.T.1, DASSANAYAKE D.L.B.2, GAMAGE L.N.3 1Senior Registrar in Radiology, 2Senior Registrar in Chest Medicine, 3Consultant Radiologist. Teaching Hospital, Kandy, Sri Lanka
Introduction RP is a rare multisystemic disorder characterized by inflammation of the cartilaginous structures of the body. In RP airway involvement is seen 50% of cases and found to be the major cause of deaths related to RP. 50% of deaths due to RP are due to respiratory involvement( 3,4). Men and women are affected equally. The average age at presentation is 47 years. The diagnosis is established when any three of the following clinical features are present: bilateral auricular chondritis, nonerosiveseronegative inflammatory arthritis, nasal chondritis, ocular inflammation, respiratory tract chondritis, or audiovestibular damage (1). No specific histopathologic finding is considered pathognomonic for relapsing RP. When the clinical picture is clear, biopsy is unnecessary (2). In less straightforward cases, however, biopsy may be required to exclude other diseases, including infection.
History and Examination • A 40 y old male farmer • Cough and pleuritic chest pain for 02 weeks • Fever for 04 days . • No haemoptysis, wheeze, loss of appetite or loss of weight • Clinical examination was unremarkable
Investigations • FBC- leukocytosis -15000mm-3 • ESR -123/1st hr.,145/1st hr • CXR -normal. • Sputum for acid fast bacilli – negative • Mantoux -non-reactive. • Renal & liver functions -normal • Blood picture – unremarkable • ANA & rheumatoid factor -negative.
02 weeks later Developed pain in throat, nose and both ears chest wall pain. Examination - tenderness of ears, nose, anterior neck and costochondral junctions Lung function tests-obstructive lung defect
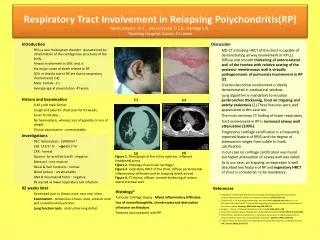
Figure 1; Photograph of the inflamed(reddened)pinaof the right ear.
HRCT - Chest Figure 1; Axial CT scan of chest reviles diffuse, smooth thickening of antero- lateral tracheal wall.
Figure 4; Axial CT scan of the chest reveals diffuse inflammatory infiltrates and expiratory HRCT shows focal air trapping(black arrow). peribronchial soft tissue thickening, consistent with RP.
Imaging Findings CT scan of the chest diffuse, smooth thickening of antero- lateral tracheal wall. HRCT scan of the chest diffuse peribronchial inflammatory infiltrates and expiratory HRCT shows focal air trapping. These findings are consistent with RP
Histology Nasal septal biopsy ; there is a mixed inflammatory infiltrate (lymphocytes, plasma cells, neutrophils, occasional eosinophils) extending into cartilage. Interface between cartilage and adjacent soft tissue is blurred. Cartilage demontratesloss of normal basophilia, loss of chondrocytes and destruction of lacunar architecture. Features are consistent with RP.
Discussion • MD-CT including HRCT of the chest is capable of demonstrating air way involvement in RP (1). Diffuse and smooth thickening of antero-lateral wall of the tracheal wall with relative sparing of the posterior membranous wall is virtually thought to be pathognomonic of pulmonary involvement in RP. Demonstration of traceo-bronchial involvement with mediastinal windowing and peribronchial thickening, focal air trapping and patchy atalectasis with lung algorhythm is very much important in making diagnosis (2).These features were well appreciated in this case too.
The most common CT finding of lower respiratory tract involvement by relapsing polychondritis is increased airway wall attenuation seen in (100%). The degree of increased attenuation ranged from subtle to frankly calcified. Progressive cartilage calcification is a frequently reported feature of relapsing polychondritis (6). In our case no cartilage calcification was found but higher attenuation of airway wall was noted.
Air way luminal narrowing was noted 80% of some case series but significant narrowing (25%of normal caliber) was not seen our patient(6). As in our case air trapping on expiration is well described as a key feature of RP and expiratory CT is considered to be mandatory as part of imaging.
CT is an important tool in the evaluation of patients with known or suspected RP. In patients with known disease, CT is useful for confirming intrathoracic involvement and for routine follow-up to assess progression of disease. Tillie-Leblond et al. (5) reported that CT was better than fiberopticbronchoscopy in identifying airway stenoses and tracheal wall alterations in the early stages of disease. In patients without a known diagnosis of RP, the finding of diffuse increased airway wall attenuation and thickening at CT, with or without stenosis, suggests the diagnosis and should prompt a careful rheumatologic assessment (1, 2).
References 1. McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine 1976;55:193–215 2.Trentham DE, Le CH. Relapsing polychondritis. Ann Intern Med 1998;129:114–122Keren S. Lee, MD, Armin Ernst, MD, David E. Trentham, MD, Relapsing Polychondritis: Prevalence of Expiratory CT Airway Involvement, Radiology RSNA 2006, Aug; 240; 565-571. 3.Gergely P., Poor G. , Relapsing Polychodritis, Pract Best Clin 2004;18:723-738. 4.Armin Ernst, SamaanRafique, Phillip Boiselle., Relapsing Polychondritis ,CHEST2009; 135: 1024-1030. 5.Tillie-Leblond I, Wallaert B, Leblond D, et al. Respiratory involvement in relapsing polychondritis: clinical, functional, endoscopic, and radiographic evaluations. Medicine1998;77:168–176 6. Jeffrey V. Behar ,Yo-Won Choi, et al. Relapsing Polychondritis Affecting the Lower Respiratory Tract, AJR:, January 2002;178:173-177.
Respiratory Tract Involvement in Relapsing Polychondritis(RP)MUTHUNAYAKE M.T.1, DASSANAYAKE D.L.B.2, GAMAGE L.N.3 1Senior Registrar in Radiology, 2Senior Registrar in Chest Medicine, 3Consultant Radiologist. Teaching Hospital, Kandy, Sri Lanka Introduction RP is a rare multisystemic disorder characterized by inflammation of the cartilaginous structures of the body. Airway involvement is seen 50% of cases and found to be the major cause of deaths related to RP. 50% of deaths due to RP are due to respiratory involvement( 3,4). Men and women are affected equally. The average age at presentation is 47 years. History and Examination A 40 y old male farmer Cough and pleuritic chest pain for 02 weeks Fever for 04 days . No haemoptysis, wheeze, loss of appetite or loss of weight Clinical examination was unremarkable Investigations FBC- leukocytosis -15000mm-3 ESR - 123/1st hr.,145/1st hr CXR - normal. Sputum for acid fast bacilli – negative Mantoux - non-reactive. Renal & liver functions - normal Blood picture – unremarkable ANA & rheumatoid factor - negative. Rx started as lower respiratory tact infection 02 weeks later Developed pain in throat, nose and both ears chest wall pain. Examination - tenderness of ears, nose, anterior neck and costochondral junctions Lung function tests-obstructive lung defect Figure 1; Photograph of the inflamed(reddened)pina of the right ear. Figure 2; a; CT thorax; diffuse, smooth thickening of antero- lateral tracheal wall. b; HRCT scan of the chest diffuse peribronchial inflammatory infiltrates and expiratory HRCT shows focal air trapping. Histology Nasal septal biopsy ; there is a mixed inflammatory infiltrate Cartilage demontratesloss of normal basophilia, loss of chondrocytes and destruction of lacunar architecture. Features are consistent with RP. Discussion MD-CT including HRCT of the chest is capable of demonstrating air way involvement in RP (1). Diffuse and smooth thickening of antero-lateral wall of the tracheal wall with relative sparing of the posterior membranous wall is virtually thought to be pathognomonic of pulmonary involvement in RP. Demonstration of traceo-bronchial involvement with mediastinal windowing and peribronchial thickening, focal air trapping and patchy atalectasis with lung algorhythm is very much important in making diagnosis (2).These features were well appreciated in this case too. The most common CT finding of lower respiratory tract involvement by RP is increased airway wall attenuation seen in (100%). The degree of increased attenuation ranged from subtle to frankly calcified. Progressive cartilage calcification is a frequently reported feature of RP(6). In our case no cartilage calcification was found but higher attenuation of airway wall was noted. As in our case air trapping on expiration is well described as a key feature of RP and expiratory CT is considered to be mandatory as part of imaging. References 1. McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine 1976;55:193–215 2. Trentham DE, Le CH. Relapsing polychondritis. Ann Intern Med 1998;129:114–122Keren S. Lee, MD, Armin Ernst, MD, David E. Trentham, MD, Relapsing Polychondritis: Prevalence of Expiratory CT Airway Involvement, Radiology RSNA 2006, Aug; 240; 565-571. 3. Gergely P., Poor G. , Relapsing Polychodritis, Pract Best Clin 2004;18:723-738. 4. Armin Ernst, SamaanRafique, Phillip Boiselle., Relapsing Polychondritis ,CHEST2009; 135: 1024-1030. • 5. Tillie-Leblond I, Wallaert B, Leblond D, et al. Respiratory involvement in relapsing olpychondritis: • clinical, functional, endoscopic, and radiographic evaluations. Medicine1998;77:168–176 6. Jeffrey V. Behar ,Yo-Won Choi, et al. Relapsing Polychondritis Affecting the Lower Respiratory Tract, AJR:, January 2002;178:173-177.





