Download
1 / 30
310 likes | 747 Vues
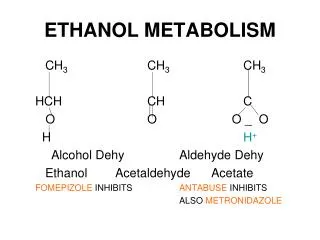
Ethanol Pharmacokinetics, Metabolism and Forensic Aspects. The goal of this lecture is to describe the biochemical pathways which play a role in the metabolism of ethanol.

E N D
Ethanol Pharmacokinetics, Metabolism and Forensic Aspects • The goal of this lecture is to describe the biochemical pathways which play a role in the metabolism of ethanol. • The pathways will be described with respect to the enzymes involved, the factors which regulate the overall flux through the pathway, and how these pathways impact on normal physiological pathways involved in metabolism of nutrients and drugs. • The effects of chronic ethanol consumption on ethanol and acetaldehyde metabolism will be discussed, including factors which may be responsible for metabolic tolerance. • Factors which influence the absorption and the elimination of ethanol will be discussed.
Why is Understanding Pathways of Ethanol Metabolism Important? • Learn how the body disposes of ethanol and its metabolites. • Discern some of the factors which influence this process. • Learn how ethanol influences the metabolism of nutrients and drugs, and modulates the therapeutic effectiveness of drugs. • May learn how ethanol damages various organs. • May help to identify individuals who are at increased or decreased risk for alcohol toxicity.
Some Suggested Causes for Alcohol Toxicity Redox state changes (↓NAD+/NADH) Acetaldehyde formation Mitochondrial damage Cytokine formation Kupffer cell activation Immune response Membrane effects Hypoxia Oxidative stress
Distribution of Ethanol in the Body • The equilibrium concentration of ethanol in a tissue depends on the relative water content of that tissue. The rate of equilibration of ethanol with a tissue depends on Permeability (water content) Rate of blood flow Mass of the tissue • Ethanol is practically insoluble in fats and oils, although like water, it can readily pass through biological membranes. • Ethanol distributes from the blood into all tissues and fluids in proportion to their relative content of water. The concentration of ethanol in a tissue is dependent on the relative water content of the tissue, and reaches equilibrium quickly with the concentration of ethanol in the plasma. There is no plasma protein binding for ethanol.
Factors Affecting Ethanol Absorption 1. Concentration of ethanol 2. Blood flow at site of absorption 3. Irritant properties of ethanol 4. Rate of ingestion 5. Type of beverage 6. Food Absorption of ethanol from the duodenum and jejunum is much more rapid than from the stomach, hence the rate of gastric emptying is an important determinant of the rate of absorption of orally administered ethanol.
First Pass Metabolism of Ethanolin the Stomach Some of the ethanol which is ingested orally does not enter the systemic circulation but may be oxidized in the stomach by ADH isoforms such as s- (or m)-ADH and class I and class III ADH. This first pass metabolism could modulate ethanol toxicity since its efficiency determines the bioavailability of ethanol.
< 10 % ethanol excreted in breath, sweat and urine. ~ 90 % ethanol removed by oxidation. Most of this ethanol oxidation occurs in the liver. Ethanol cannot be stored in the liver. 5. No major feedback mechanisms to pace the rate of ethanol metabolism to the physiological conditions of the liver cell. General Scheme for Ethanol Oxidation
Kinetics of Ethanol Elimination In-vivo 1 2 3 4 Co BAC or BrAC b Time [Hours]
Constantaa b1b1 b2b2 b3b31g1 g2g2 pp Km NAD+,mM 13 7.4 180 530 7.9 8.7 14 Km ethanol, mM 4.2 0.049 0.94 24 1 0.63 34 Ki 4-methylpyrazole, mM 1.1 0.13 - 2.1 0.1 - 2000 Vmax min-1 27 9.2 400 300 87 35 20 pH-optimum 10.5 10.5 8.5 7.0 10.5 10.5 10.5 Alcohol Dehydrogenase Physiological Function? Isoforms-Why so many? Localization-consequence on liver function. Development. Crabb et. al 1987 & Bosron et. al 1993
Factors Modifying the Ethanol Elimination Rate There is a 3-4 fold variability in the rate of ethanol elimination by humans because of genetic and environmental factors, including sex, age, race, food, biological rhythms, exercise, alcoholism, and drugs.
Alcohol Dehydrogenase • Control of ADH activity is complex • dissociation of the product NADH is rate limiting step. • Subject to product inhibition by NADH and acetaldehyde. • Subject to substrate inhibition by high concentrations of ethanol.
Frequency of ADH Allelesin Racial Populations Bosron et. al. 1993 & Crabb 1995
Hepatic Redox State • ADH and ALDH reactions use NAD+ and produce NADH. • Cytosolic Redox State. • Mitochondrial Redox State. • Effects on Liver Metabolism.
Reoxidation of NADH Generated by the ADH Reaction • There is a need to reoxidize NADH back to NAD+. • Cytosolic pathways are not sufficient. • NADH must be reoxidized by the mitochondrial • electron transfer pathway shown below.
Catalase-Dependent Oxidationof Ethanol CH3CH2OH + H2O2 CH3CHO + 2H2O Catalase, a heme enzyme, is found in the peroxisomal fraction of the cell. This is an important antioxidant enzyme since it normally catalyzes the removal of H2O2. H2O2 + H2O2 2H2O + O2
Microsomal (Cytochrome P450) Oxidation of Ethanol NADPH + CH3CH2OH NADP+ + CH3CHO + 2H2O CYP2E1 - Function Role in Ethanol Oxidation Inducibility CYP2E1 + O2 + H+
Cytochrome P450 2E1 (CYP2E1) • Minor pathway of ethanol metabolism, produces acetaldehyde, and 1-hydroxyethyl radical • Alcohol-drug interaction • Activates toxins: acetaminophen, benzene, CCl4, halogenated hydrocarbons, halothane • Activates pro-carcinogens: nitrosamines, azo compounds • Activates O2 to produce ROS: O2˙- and H2O2
Alcohol-Drug Interactions:The CYP2E1 system can explain • Increased sensitivity of active drinkers to certain drugs. • Resistance of alcoholics, in the absence of ethanol, to certain drugs. • Increased toxicity of certain chemicals in alcoholics. • Ethanol-dependent oxidative stress.
Regulation of CYP2E1 expression • Transcriptional- Birth, High blood alcohol • Translational- Pyridine • mRNA Stabilization- Diabetes • Protein Stabilization- Ethanol, low mol.wt. “inducers” e.g. Pyrazole, DMSO, Acetone
Metabolic Adaptation (Tolerance) Besides CNS adaptation, alcoholics (in the absence of liver disease) often display an increased rate of blood alcohol clearance. This is called metabolic tolerance or adaptation. Suggested mechanisms include: 1. Induction of ADH. 2. Increased shuttle capacity. 3. Increased reoxidation of NADH. 4. Induction of CYP2E1. 5. Release of cytokines or prostaglandins which increase oxygen consumption by the hepatocytes.
Zonal Metabolism of Ethanol in the Hepatic Acinus Liver injury after chronic ethanol treatment originates in the perivenous zone of the hepatic lobule. Possible factors to explain this include: 1. Oxygenation. 2. Ethanol metabolism by ADH. 3. Acetaldehyde metabolism by ALDH. 4. CYP2E1. 5. Antioxidant levels.
Other Possible Pathways of Ethanol Metabolism • Conjugation reactions • Fatty acid ethyl esters • Oxygen radical-dependent reactions
Acetaldehyde Metabolism The balance between the various ADH and ALDH isoforms regulates the concentration of acetaldehyde, which is important as a key risk factor for the development of alcoholism. 1. Isoforms of ALDH. 2. Effects of Alcohol Consumption. 3. Alcohol-aversive drugs. 4. Significance of Acetaldehyde Removal.
Forensic Considerations • Time lag • Ethanol elimination rates • Partition ratio • Fluctuations and anomalies • Back extrapolation procedures • Other factors.
Breath Alcohol Levels Breath-Alcohol [mg per 230 L] Time [Hours]
Questions for Consideration • What limits and regulates ethanol metabolism in vivo? • What is the mechanism(s) responsible for metabolic tolerance? • Is it ethanol per se, or ethanol-derived metabolites which play a key role in organ damage? What might be the consequences of attempting to accelerate ethanol metabolism? • What is the significance of first pass metabolism by the stomach? • What is the role, if any, of the various ADH in oxidation of endogenous substrates, ethanol metabolism and ethanol toxicity? The hypothesis that ethanol or acetaldehyde inhibit the oxidation of physiologically important endogenous substrates of ADH and ALDH (e.g. retinol retinal retinoic acid) and that this may contribute to the adverse actions of ethanol requires further studies.
Questions for Consideration • Can the various ADH and ALDH or polymorphic forms of CYP2E1 be of predictive value or serve as markers to identify individuals who are susceptible to developing alcoholism? Can non-invasive probes be developed to measure the various isoforms present? • Are there population and gender differences in rates of ethanol elimination, and if so, are such differences explained by the varying ADH and ALDH isoforms present in that population? • What controls the expression of the various isoforms at transcriptional level, and are there posttranscriptional modifications? What dictates the turnover of these enzymes which may be important in regulating the amount of active enzyme present in the cells e.g. CYP2E1.
Questions for Consideration • Why are calories from ethanol less efficient in providing energy than calories from other nutrients? • What is the mechanism by which food increases ethanol metabolism? • What role, if any, does acetate play in the metabolic actions of ethanol? • Can we build appropriate models and rate equations to kinetically describe the process of ethanol elimination under various conditions?