Demyelinating Diseases
Demyelinating Diseases. DR. Abdulkader Daif, MD Consultant and Professor of Neurology KKUH, Faculty of medicine. Group 341-2014. Introduction to Multiple Sclerosis (MS). Chronic autoimmune disease Progressive disease Involves Immune System & Neurological System


Demyelinating Diseases
E N D
Presentation Transcript
Demyelinating Diseases DR. Abdulkader Daif, MD Consultant and Professor of Neurology KKUH, Faculty of medicine Group 341-2014
Introduction to Multiple Sclerosis (MS) • Chronic autoimmune disease • Progressive disease • Involves Immune System & Neurological System • Multifocal areas of demyelination • Disrupts ability of the nerve to conduct electrical impulses • Leads to symptoms
Classification of the Demyelinating diseases: Multiple sclerosis: A- Chronic relapsing encephalomyelopathic form. B- Acute multiple sclerosis. C- Neuromyelitis optica. Diffuse cerebral sclerosis (encephalitis periaxalis diffuse) or Schilder and concentric sclerosis of Balo. Acute disseminated encephalomyelitis. A- Following measles, rubella & influenza. B- Following rabies or smallpox vaccination. Acute and subacute necrotizing hemorrhagic encephalitis. A- Acute encephalopathic form (hemorrhagic leukoencephalitis of Hurst) B- Subacute necrotic myelopathy C- Acute brain purpura(acute pericapillary encephalorrhagia)
Types of MS • Relapsing-remitting MS (RRMS) • Affects 85% of newly diagnosed • Attacks followed by partial or complete recovery • Symptoms may be inactive for months or years • Secondary-progressive MS (SPMS) • Occasional relapses but symptoms remain constant, no remission • Progressive disability late in disease course
Types of MS • Primary-progressive MS (PPMS) • Affects approximately 10% of MS population • Slow onset but continuous worsening condition
Multiple Sclerosis Subtypes(Coyle P, CNS News 2002; adapted from Lublin F, et al Neurology 1996)
Epidemiology of MS • Age onset 20 – 50 years old • Women are 2 times more likely to develop MS • 500,000 cases in US • Over 2.5 million people around the world • More prevalent whites of northern European ancestry
Multiple SclerosisAn Immunogenetic Disease Environmental Factors Demographics/Epidemics Microbial Agents EBV Vitamin D • Genetic Predisposition • Twins studies • HLA-DR2 (DRß1*1501)(antigen presentation) • IL-2Ra • (regulatory T-cells) • IL-7Ra • (memory T-cells) • ST8SIA1 Immune Dysregulation MS Graphic courtesy of Dr. Suhayl Dhib-Jalbut.
MS 1. Research into the Causes of MS Environmental factors Genetic factors Immunological factors
Other Factors Influencing MS • Vitamin D deficiency • Vitamin D3 receptor important in immune function • Present on T regulator cells • Infectious Mono/EBV • 99% of MS patients have EBV titers • Usually higher than in HC • Pseudo follicles in meninges containing B cells showing ENA antigen • EBER RNA found in inflammatory lesions • Protein stimulates Toll 3 receptors which release proinflammatory interferons • In inflammatory lesions T cells found surrounding B cells containing ENA antigen • Genetics • HLA DRB2 *1503 allele 2x risk factor • IL 2 receptor • IL 7 receptor • 50 new candidates genes each with low risk factors
Symptoms of MS • Vision problems • Numbness • Difficulty walking • Fatigue • Depression • Emotional changes • Vertigo & dizziness • Sexual dysfunction • Coordination problems • Balance problems • Pain • Changes in cognitive function • Bowel/bladder dysfunction • Spasticity
Multiple SclerosisPathophysiology • Disease process consists of loss of myelin, disappearance of oligodendrocytes, and proliferation of astrocytes • Changes result in plaque formation with plaques scattered throughout the CNS
Multiple SclerosisPathophysiology • Initially the myelin sheaths of the neurons in the brain and spinal cord are attacked, but the nerve fiber is not affected • Patient may complain of noticeable impairment of function • Myelin can regenerate, and symptoms disappear, resulting in a remission
Multiple SclerosisEtiology and Pathophysiology • Myelin can be replaced by glial scar tissue • Without myelin, nerve impulses slow down • With destruction of axons, impulses are totally blocked • Results in permanent loss of nerve function
MS Disease Timeline(Fox RJ, Sweeny PJ, Cleveland Clinic, May 2002)
* CIS Natural History of MSClinical and MRI Measures Relapses/Disability MRI Activity MRI T2 Burden of Disease Secondary Progressive MS Axonal Loss Relapsing-Remitting MS Preclinical Disability Time Trapp BD, et al. Neuroscientist. 1999;5:48-57. Reprinted with permission from Sage Publications.
RECENT LESIONS LATER OLD LESION • Relatively acellular • More clearly demarcated. • Bare axons are surrounded by astrocytes. • Myelin destruction • Relative axon sparing • Perivenous infiltration with MNP • Breakdown of BBB Astrocyte proliferation
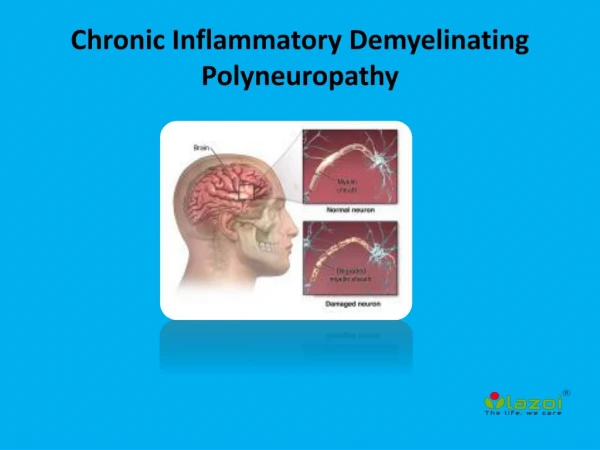
The Biology of MS How does the CNS work? Nerve Cell Messages travel to and from the CNS through nerve cells3 Myelin surrounds the nerve fibers, protecting them like the coating of a wire1 Myelin Nerve fibers (or axon) Cell body Nerve fibers (or axon) Myelin
How does MS affect the CNS? The Biology of MS In MS, cells of the immune system attack myelin and can cause permanent damage Areas where myelin has been damaged interrupt communication Exposed nerve fibers are severed, causing permanent damage Nerve Cell
Inflammation and Axonal Transection Main Clinical Outcome Disease Stage Main Component Early Inflammation and demyelination Relapses Late Atrophy, axonal loss, and Disability increasing tissue destruction (less Gd-defined inflammation, demyelination ongoing)
The Biology of MS How is MS monitored? MRI showing no signs of damage MRI showing an active lesion* MRI showing permanent damage Magnetic Resonance Imaging (MRI) detects areas of inflammation (active lesions) and areas of permanent damage in the brain1 Active lesion Permanent damage • These images may also help detect “silent” damage (lesions detected by MRI that do not result in symptoms)1 • The impact of this damage depends on the destructiveness of the lesion and where itis located *The exact relationship between MRI findings and the clinical status of patients is unknown.
Diagnosis of MS • Clinically definite MS must meet criteria for1 • Dissemination in space • Dissemination in time • A single episode of MS-like symptoms (clinically isolated syndrome [CIS]) will not meet these criteria • But if MS is likely based on MRI, it still should be treated like MS • Delaying treatment may be missing an important window of opportunity to delay the onset of irreversible disability • Requires close monitoring over time to confirm diagnosis 1. Polman CH, et al. Ann Neurol. 2005;58:840-846.
Revised McDonald Criteria for Dissemination in Time • At least 1 of the following • A 2nd clinical episode • A Gd-enhancing lesion detected ≥3 months after onset of initial clinical event • Located at a site different from the one corresponding to the initial event • A new T2 lesion detected any time after a reference scan that was performed at least 30 days after the onset of an initial clinical event • Thus, it is not always necessary to wait for 2 attacks to diagnose MS. A first attack plus changes on MRI may be enough Polman CH, et al. Ann Neurol. 2005;58:840-846.
Revised McDonald Criteria for Dissemination in Space • At least 3 of the following: • ≥1 Gd-enhancing brain or spinal cord lesion or ≥9 T2 hyperintense brain and/or spinal cord lesions of ≥3 mm in size if none of the lesions are Gd-enhancing • ≥1 brain infratentorial lesion or spinal cord lesion ≥3 mm in size • ≥1 juxtacortical lesion ≥3 mm in size • ≥3 periventricular lesions ≥3 mm in size Polman CH, et al. Ann Neurol. 2005;58:840-846.
Clinical Features Suggestive of MS • Onset between 15-50 years • Blurred or double vision • Lhermitte’s sign • Fatigue • Heat sensitivity • Bladder symptoms • Cognitive or affective changes
Clinical Features • Sensory Symptoms • Numbness & Paraesthesia • Impaired vibration & Joint position sensation • Lhermitte’s Sign ( Shock-like sensation in the limb) • Dysaesthesia + Sensory loss to pain & Temp.
Clinically Isolated Syndromes • Transverse Myelitis • Risk factors for MS • Incomplete transverse myelitis • Asymmetric motor or sensory findings • Brain MRI lesions • Abnormal CSF • Abnormal VER and SSEPs • Others (Brainstem, Cerebellum)
Optic Neuritis: Clinical Features • Inflammatory demyelination of one or both optic nerves • Pain around one eye • Blurred vision • Loss of color vision • Swollen optic disc( Papillitis) • Visual field defect • Diplopia & Vertigo
Clinically Isolated Syndromes • Optic Neuritis • Risk factors for MS (60-75%) • History of minor neurologic sxs • Unilateral optic neuritis • Brain MRI lesions • Abnormal CSF • Abormal VERs
Diseases to rule out • Viral infections • Lyme disease • B12 deficiency • CVA • Lupus • Rheumatoid arthritis • Other connective tissue disorders • Vasculitis • Syphilis • Tuberculosis • Neurobrucellocis • HIV • Sarcoidosis
Typical MRI Lesions in MS Infratentorial Juxtacortical C and D: Courtesy of Daniel Pelletier, MD.
Typical MRI Lesions in MS Periventricular Spinal Cord E: Courtesy of Daniel Pelletier, MD.F: Courtesy of Tracy M. DeAngelis, MD.
Typical MRI Lesions in MS Gd-enhancing Corpus Callosum A and B: Courtesy of Tracy M. DeAngelis, MD.
Distinguishing NMO from MS NMO MS Courtesy of Bruce A.C. Cree, MD, PhD, MCR Courtesy of Tracy M. DeAngelis, MD
Other Diagnostic Tools for MSVisual Evoked Potentials (VEPs) • Provides evidence of a lesion associated with visual pathways • Positive if shows delayed but well-preserved wave forms • Abnormal VEP is not specific for MS • Can help establish dissemination in space
LABORATORY ASSISTED DIAGNOSIS MS lesions in various stages can now be seen on MRI Cerebrospinal fluid analysis can identify immunoglobulin synthesis Evoked potentials can demonstrate clinically and even MRI silent lesions
Other Diagnostic Tools for MSCSF Analysis • Positive if oligoclonal IgG bands present but absent from corresponding serum sample or IgG index is elevated • Sensitive but not specific: other causes of CNS inflammation can yield similar findings • Lymphocytic pleocytosis is rarely >50/mm3 • Protein levels rarely exceed 100 mg/dL • Elevated myelin basic protein is not pathognomonic for MS
Neurophysiological Investigations No diagnostic test. Only support the clinical suspicion. • Visual evoked potential(VEP): in optic nerve the latency of the large positive wave is delayed . the amplitude may also be reduced. • Somatosensory evoked response (SSEP) may detect central sensory pathway lesion. • Brain stem auditory evoked potential (BAEP) may detect brain stem lesion.
Therapeutic Goals in MS • Prevent disability • Prevent relapses • Relieve symptoms • Maintain well-being • Optimize quality of life An effective therapy administered early in the disease course can impact all of these goals
approved In phase II Filed In phase III Existing Therapies and Emerging Therapies for MS 2005 2006 2007 2010 2011 2012 2013 Orals Injectables BG 12 Oral Fumarate Oral Cladribine Rebif Teriflunomide Betaseron FTY 720 Laquinimod Copaxone SB683699 Fampridine ambulation indication? Avonex IV Novantrone IV Campath Tysabri Rituximab II - RRMS; III - PPMS Generic Mitoxantrone (oncology) (MS) Daclizumab MLN1202 MBP 8298
Second Second-Line MS Therapies • Mitoxantrone • Natalizumab • Generally indicated for persons with suboptimal response to first-line agents • Require intravenous infusion • Associated with life-threatening adverse events
Oral MS Therapies • Fingolimod • Fumarate • Teriflunomide • Laquinimod • Cladribine