Download
1 / 20
200 likes | 357 Vues
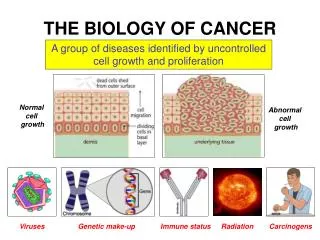
MBBS Cancer Biology Module 2006. Tumour Vasculature and Therapeutic Strategies Barbara Pedley. TUMOUR ANGIOGENESIS. What is tumour angiogenesis? Why is it important? Why is it a good target for therapy?

E N D
MBBS Cancer Biology Module 2006 Tumour Vasculature and Therapeutic Strategies Barbara Pedley
TUMOUR ANGIOGENESIS • What is tumour angiogenesis? • Why is it important? • Why is it a good target for therapy? • What examples are there of cancer therapies that selectively target the vasculature?
Tumour Angiogenesis • Formation of new vessels from pre-existing vasculature • Required for tumour growth (>1mm3) and metastasis Cell Differentiation Cell Migration tumour Angiogenic Stimulus Cell Division BM & ECM Breakdown
Angiogenic Switch Initiated by switch in balance from anti- to pro-angiogenic factors
Differences between tumour and normal vessels • High endothelial cell proliferation rate • (3-13 v 47-2000 day) • Distorted and chaotic architecture, with • sluggish blood flow, shunts and dead ends • Leaky vessels • Frequently results in regions of hypoxia
Normal v tumour vessels normal tumour Well Oxygenated
BUT: Tumour Vessel Abnormalities are Targetable • Advantages of Vessel v Tumour Cell Targeting • Rapidly dividing • Accessibility • 1 capillary supports many tumour cells • No drug resistance • Applicable to all solid tumours Tumour vessels
TUMOUR BLOOD VESSELS: A TARGET FOR NOVEL THERAPEUTICS I. Endogenous inhibitors II. Small molecule inhibitors & antibodies III. Antivascular drugs All in clinical trials http//cancertrials.nci.nih.gov/news/angio/table.html Kerbel R & Folkman J. Clinical translation of angiogenesis inhibitors. Nature Reviews 2: 727-739, 2002. Falm E. Angiogenic inhibitors in clinical development. BJC 90: 1-7, 2004. Neri D & Bicknell R (2005). Tumour vascular targeting. Nature Reviews/ Cancer 5: 536-446.
I. Endogenous inhibitors eg angiostatin Saline Angiostatin Effect of angiostatin on corneal vessel proliferation
II. Small molecule inhibitors & antibodies • Inhibitors of matrix metalloproteinases • block ECM breakdown • Anti-integrin antibodieseg Vitaxin • block endothelial cell adhesion & survival • Anti-VEGF antibodies eg Avastin • blocks growth factor function & signalling The first anti-angiogenesis strategy to be licenced by the FDA to treat human cancer (2004)
VASCULAR ENDOTHELIAL GROWTH FACTOR (VEGF) • Expressed at high levels by many tumours • Reacts with receptors on vascular endothelium • Functions essential for tumour growth: • promotes angiogenesis • promotes vascular permeability • Clinical importance • high VEGF levels in tumour and plasma frequently • correlate with poor prognosis
Bevacizumab (AvastinTM) - Survival IFL: bolus 5-FU 500 mg/m2 leucovorin 20 mg/m2 irinotecan 125 mg/m2 Expensive! Gerber & Ferrara, Cancer Res 65: 671-680, 2005
V N 24 h post drug • III Antivascular Drugs eg.Combretastatin • tubulin binding agent/colchicine binding site • targets angiogenic and established tumour vessels • inhibits tumour blood flow • destroys all but the tumour rim V V Untreated
RADIOIMMUNOTHERAPY CT scans showing response Radionuclide 131I Antibody before Bystander effect Antigen eg CEA DNA strand breaks Cell death after Tumour cell
Basis of Combined Therapies V N Combretastatin 24h Antibody Blood vessel distribution Therapy: RIT + CA4-P
A Phase I/II Trial of Radioimmunotherapy with 131I-A5B7 anti-CEA Antibody in Combination with CA4-P for Advanced Gastrointestinal CarcinomaSTUDY PH1-092
Summary of Tumour Vessels Tumour v normal blood vessels: • High endothelial cell proliferation rate • Abnormal morphology, biochemistry and physiology • Development of hypoxia leads to: • increased angiogenesis and tumour growth • tumour resistance to conventional therapies • altered gene expression • increased metastatic potential • However...…..
Summary of Antivascular Therapy • The abnormal vasculature of solid tumours provides exciting new targets for therapy • Low drug resistance v tumour cells • Low toxicity • Long-term dosing frequently required • Combined therapies (eg anti-vascular + anti-tumour cell) will frequently be required to eradicate tumours