
Facial Affect Misattributions in Schizophrenia: Social Cognitive Biases in Paranoid Symptoms
This study explores how individuals with schizophrenia misinterpret facial emotions, particularly in relation to paranoid symptoms. It investigates the connection between affect misattributions and specific schizophrenia symptoms. The research suggests that people with paranoid symptoms tend to make more misattributions related to interpersonal threat, such as anger and disgust. The findings align with social cognitive models of paranoia, indicating biases in social information processing among those with paranoid symptoms. The study analyzes affect recognition abilities and psychiatric symptoms in a sample of individuals diagnosed with a schizophrenia spectrum disorder. By examining facial affect misattributions, the study aims to shed light on the social cognitive biases present in schizophrenia.

Facial Affect Misattributions in Schizophrenia: Social Cognitive Biases in Paranoid Symptoms
E N D
Presentation Transcript
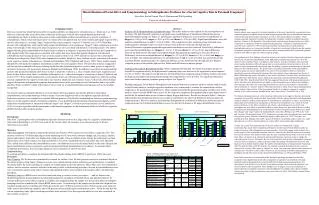
Misattributions of Facial Affect and Symptomatology in Schizophrenia: Evidence for a Social Cognitive Bias in Paranoid Symptoms? Jason Peer, Rachel Penrod, Thea L. Rothman and Will Spaulding University of Nebraska-Lincoln • INTRODUCTION • Previous research has found that facial affect recognition abilities are impaired in schizophrenia (i.e., Morrison et al. 1988). However, relatively little research has been conducted on the types of facial affect misattributions persons with schizophrenia are likely to make on these tasks and the relationships of these misattributions to specific symptoms of schizophrenia. That is, when making an error on a facial affect recognition task how often would a participant respond with a specific affect type (i.e. selecting “anger” instead of the correct response “surprise”)? Garfield et al. (1987) found that persons with schizophrenia made significantly greater misattributions of an emotion as “disgust” when compared to a control group. Interestingly, in this study, poor affect recognition was also correlated with defensive self-enhancement. The authors suggest that the greater misattribution of disgust may be related to a diagnosis of paranoia but did not test this hypothesis in their original study. This suggestion is consistent with studies that have shown that patients diagnosed with paranoid schizophrenia tend to judge pictures of faces as more negative (Smari et al. 1994) and tend to express more unfavorable feelings about the picture (Izard 1959) when compared to controls. Intuitively, these findings are also consistent with current social cognitive models of paranoia (i.e., Bentall and Kinderman 1998; Chadwick and Trower 1997). These models suggest that patients with paranoid symptoms demonstrate a number of social cognitive biases. Research has found an exaggerated self-serving bias combined with a personalizing attribution bias (attributing negative events to other people as opposed to situations) in persons with persecutory delusions (Bentall and Kinderman 1998). In addition, research has demonstrated that persons with paranoid symptoms show biases in their evaluations of others (i.e., they evaluate others more negatively) and biases in their beliefs about others’ evaluations of themselves (i.e., others hold negative evaluations of them) (Chadwick and Trower 1997). These models propose that social cognitive biases are utilized to protect against depressive affect by seeking external explanations for negative events and in turn result in attentional and evaluative biases. Collectively, these findings suggest that patients with paranoid symptoms demonstrate biases in the processing of social information and it is possible that these biases would be evident in the types of errors made on social information processing tasks such as facial affect recognition. • The present study investigated differences in overall facial affect recognition, the specific pattern of facial affect misattributions, and symptomatology within a sample of persons diagnosed with a schizophrenia spectrum disorder. Exploratory analyses were conducted to evaluate different patterns of facial affect misattributions based on symptomatology. Based on social cognitive models of paranoid symptoms, it was predicted that participants with paranoid symptoms would make more misattributions of interpersonal threat (“anger” and “disgust”). Based on previous research (Lewis and Garver 1995), it was also hypothesized that participants with paranoid symptoms would demonstrate better facial affect recognition abilities than the other symptom groups. • METHOD • Participants • Data from 72 participants with a schizophrenia spectrum disorder involved in a large study of a cognitive rehabilitation intervention (Spaulding et al. 1999) were used for the current study. All measures were collected as part of the pre-intervention assessment. • Measures • Affect Recognition: Participants completed the Ekman and Friesen (1976) measure of facial affect recognition (FA). This measure consists of 110 slides depicting an actor displaying one of seven basic emotions (happy, sad, fear, anger, surprise, disgust and neutral). Each slide was displayed for eight seconds. Using a multiple-choice format, the participant was then instructed to select which emotion was depicted. Based on FA errors, misattributions for each affect type were tabulated. This yielded seven different affect misattribution scores. An additional score was calculated based on the sum of disgust and anger misattribution scores to represent a general interpersonal threat misattribution score (threat). To measure affect recognition performance, the overall percentage of correct responses on the FA was used. • Symptomatology • To evaluate psychiatric symptoms the Extended Brief Psychiatric Rating Scale (BPRS) (Lukoff et al. 1986) was used. • Procedure • Data Cleaning: The FA data was systematically screened for outliers. First, FA total percent correct was evaluated. Based on the outlier analysis using Tukey’s hinges two cases were excluded based on their extremely poor performance (3 standard deviations below the mean) resulting in a sample of 70 participants used in the analyses. Three other cases were identified as outliers, but less extreme, and were included in the analysis after a windsorizing procedure. Second, the misattribution scores were screened for outliers using Tukey’s hinges and identified outliers were included in the analysis after a windsorizing procedure. • Statistical Analyses: BPRS scores were factor analyzed using a varimax rotation procedure….. and six factors were identified (paranoid, anxiety/depression, hallucination/delusion, disorganized, blunted affect, and agitation/elation). To evaluate differences in the affect recognition variables and symptomatology the sample was divided into different symptom groupings based on a median split of each BPRS factor scores. In each analysis the sample was divided into a high and low symptom group based on a median split of the given factor score. Differences between each of these groups were analyzed with t-tests on the following variables: total FAR percent correct and the eight misattribution scores. Given the fact that this was an exploratory study alpha correction procedures were not used. Post hoc regression analyses were also conducted on the variables of interest. • RESULTS • Analysis of FA Misattributions by Symptom Group: The results indicate some support for the first hypothesis of the study. The high Paranoid symptom group made more misattributions of interpersonal threat than the low paranoid symptom group (see Figure 1). Specifically, significant differences were noted for misattributions of: disgust (t=-2.40; p=0.02), anger (t=-2.62; p=0.01) and threat (t=-3.28; p=0.002). Significant differences were also noted for misattributions of sad (t=-3.03; p=0.004). The evaluation of other symptom groups indicated some similar patterns, although results were not as robust. Some differences between the high and low Anxiety/Depression symptom groups that approached significance were also observed. Specifically, differences were noted for misattributions of: disgust (t=-1.67; p=0.10) and threat (t=-1.93; p=0.06). Some differences between the high and low Disorganized symptom groups that approached significance were also observed. Differences were noted in misattributions of: disgust (t=-1.72; p=0.09); threat (t=-1.91; p=0.06) and happy (t=-2.03; p=0.048). One significant difference for misattributions of sad (t=-2.06; p=0.048) was noted between the Agitation/Elation symptom groups. No significant differences were noted between the high and low Blunted symptom groups or between the high and low Hallucination/Delusion symptom groups. • Analysis of Overall FA Recognition Ability: When comparing the high and low Paranoid symptom groups on overall FA recognition ability, the high paranoid symptom group was observed to be significantly more impaired (t=2.91; p=0.005). The analysis of high and low Anxiety/Depression symptom groups yielded a similar result with the high anxiety/depression group demonstrating more impairment (t=2.05; p=0.05). No significant differences were noted in the remaining symptom group analyses (see Figure 2). • Post-Hoc Analyses: Given that the Disorganized and Anxiety/Depression symptom analyses yielded similar results as the Paranoid analyses, multiple regression equations were constructed to evaluate the contributions of these symptoms to the paranoid group differences. These equations included the paranoid grouping variable (used in the analyses above) and raw BPRS factor scores for the respective symptoms (disorganized and anxiety/depression) to predict the FA misattribution scores of interest (anger, disgust and threat). Results are shown in Table 1. Analyses indicated that anxiety/depression factor scores did not contribute to the observed differences between paranoid symptom groups. However, analyses indicated that disorganization contributed to differences between paranoid symptom groups for FA threat misattribution scores, but not for FA disgust or FA anger misattribution scores. • DISCUSSION • Results indicate some support for the initial hypothesis of the study. Specifically, as predicted, when comparing paranoid symptom groups the high symptom group made more misattributions consistent with interpersonal threat (disgust and anger), as well as more misattributions of sadness. These findings remained significant even after including other symptom variables in multiple regression analyses. Contrary to the hypothesis, the high paranoid symptom group demonstrated poorer affect recognition in comparison to the low paranoid symptom group. It should be noted that previous research (Lewis and Garver 1995) on paranoia and affect recognition has used the paranoid schizophrenia subtype as a categorical variable, whereas the current study utilized a specific measure of paranoid symptoms. Furthermore, the present analysis compared high and low paranoid symptom groups to each other as opposed to other symptom groups. • One explanation of these findings is based on current social cognitive theories of paranoid symptoms. Specifically, the pattern of performance of the high paranoid symptom group may have been the result of social cognitive biases. According to these theories, in order to maintain self-esteem and protect against depressive affect, this group may have demonstrated a biased perception of social stimuli as more interpersonally threatening; thus, the finding of greater misattributions of anger and disgust for this symptom group. The poorer affect recognition performance of the high paranoid symptom group can also be understood in the context of social cognitive theories of paranoia. Specifically, persons with paranoid symptoms have been found to show impairments on Theory of Mind (ToM) tasks that require the ability to infer others’ intentions (Corcoran 2001) and it has been argued that these ToM deficits may be implicated in paranoid symptoms (Bentall and Kinderman 1998; Frith 1994). Specifically, Frith (1994) has suggested that persons with paranoid delusions are able to infer their own intentions but are unable to infer the mental states of others, thus leading to false inferences that others are concealing their intentions. Likewise, the inability to decode affect may lead persons to “assume” negative affect and intentions in others, based on preexisting paranoid social cognitive biases. In fact, it has been argued that this is an adaptive response to cognitive deficits, as it is safer to assume “harmful intent” than “benevolence” (Neufield 1991 p. 252). • The former explanation however, while consistent with current social cognitive theories of paranoid symptoms, does not fully explain the data. Specifically, both the anxiety/depression and disorganized symptom analyses yielded a similar pattern of misattributions, although not as robust. An alternative, and perhaps more parsimonious explanation, is that the observed patterns were a result of overall poor performance on the affect recognition task. That is, when making errors on the FA task participants are more likely to misattribute affect as anger, disgust etc. Research in the area of affect recognition has identified patterns of misattributions on affect recognition tasks. Studies have found that “disgust” and “anger” tend to be misidentified for each other (Phillips et al. 1999) as do “fear” and “surprise” (Ekman and Friesen 1976). Furthermore, persons with schizophrenia have been found to experience greater difficulty in identifying negative affect (Bell et al. 1997). Therefore, it is possible that these findings reflect both a greater difficulty in recognizing negative affect (i.e., anger and sadness) as well as a natural tendency to confuse affect types such as anger and disgust. • To date, the current study represents one of the few studies to systematically evaluate symptomatology, facial affect recognition performance and the types of misattributions made in a sample of persons with schizophrenia spectrum disorders. The results suggest some evidence for a social cognitive bias in paranoid symptoms. However, some caveats about the results are warranted. The current analyses were unable to tease apart the types of misattributions made on an item by item basis. Thus it is unclear as to whether the pattern of performance represents a bias or simply the expected pattern of errors. Ultimately, the test of the hypothesis that persons with paranoid symptoms are more likely to misperceive affect as interpersonally threatening will depend on an item by item analysis. Future studies should evaluate the number of misattributions of interpersonally threatening affect for specific items on the FA measure. For example, counting the number of times a person misperceives “neutral” affect items as “disgust” or “anger” may represent a more accurate measure of response bias. Alternatively, affect bias could also be assessed using facial affect attentional bias paradigms used in other areas of experimental psychopathology (i.e., Mogg and Bradley 1998). • Some final comments are warranted about the findings regarding performance on the affect recognition task. Significantly poorer affect recognition recognition was identified in the high paranoid symptom grouping analysis and the high anxiety/depression grouping analysis. It is interesting to note that these were the only two symptom groups where increased symptoms were related to poorer affect recognition. These findings seem to suggest an increase in paranoia or anxiety/depression symptoms in persons with schizophrenia may impair social cognitive abilities whereas increases in other symptoms does not seem to have an effect. This finding warrants further investigation. Figure 2 Figure 1





