Download
1 / 15
150 likes | 286 Vues
Assessing the value of medicines in middle-income countries. ZF PHARMA SUMMIT 2012 , Buchares , 24 September 2012. For the sustainability of a reimbursement system , proactive and consistent policies are needed in innovative and generic sub-markets. 6. 1.

E N D
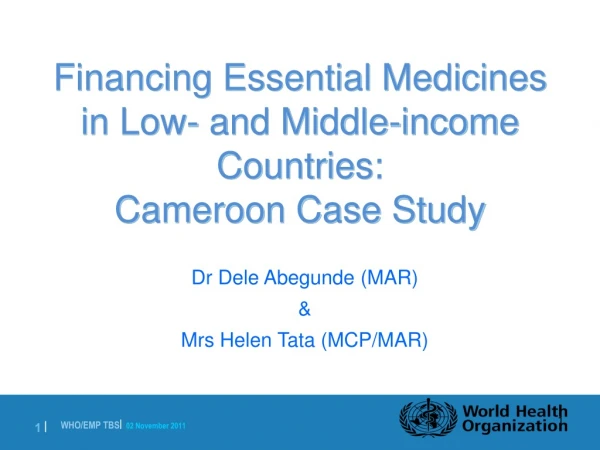
Assessing the value of medicines in middle-income countries ZF PHARMA SUMMIT 2012, Buchares, 24 September 2012
Forthesustainability of a reimbursementsystem, proactive and consistentpoliciesareneededininnovativeandgenericsub-markets 6 1 Revise effectiveness based on real-world data and restricttheuse of products with no added therapeutic value Ensureeasy and quickaccess to newgeneric medicines RECYCLE 5 2 INNOVATIVE (patent-protected) MARKETS COMPETITIVE (genericised) MARKETS Apply value-basedschemes to guarantee the optimal allocation of resources Ensure sustainablegenericpricedecrease and foster generic substitution 4 3 Admit new value-added therapies (active substances) into the formulary Eliminate inefficiencies in expenditure by identifying all sustainable cost saving potentials RECYCLE Enable the treatment of special, ‘complicated’ or rare conditions THERAPIES FOR MASS DISEASES Treat high-incidence diseases along a cost-minimisation approach NICHE THERAPIES Source: Dankó, D. – Molnár, M.P. (2012, ed.): Handbook of Pharmaceutical Reimbursement. Medicina (in press)
Pharmaceutical innovation: underlying dilemmas in the early 21st century Innovation content of new active substances introduced between 1975 and 2002 • Real therapeutic breakthrough has become extremely rare • Innovation seems to be biased towards „sellable” therapy areas, while other areas are largely neglected • BUT policy backlashes against some forms of innovation • More and more new substances cause disappointment in real-life settings Chemical structure New Already known Therapeutic value Provides progress in treatment 143 (10%) 295 (18%) Does not provide progress in treatment 201 (14%) 821 (56%) • The business model of the pharma industry is undergoing a slow but thorough transformation Source: Barral, P.E. [2004]: 28 ans de résultats de la recherchepharmaceutiquedans le monde 1975-2002. IRDES, Paris
Health technologyassessment: assessingthevalue of healthtechnologies Health technology assessment (HTA) covers all methods for • the systematic evaluationof thecomparativevalueof pharmaceutical products and otherhealthtechnologies • linked to pricing & reimbursement decisions by public and private payers • preceding to admissionto the reimbursementformulary and during formulary management.
Three main paradigms for healthtechnologyassessment (HTA) QUALITATIVE ASSESSMENT BALANCED ASSESSMENT ECONOMIC EVALUATION 2 3 1 • Based on pharmacoeconomics • Strict quantitative methods applied by dedicated HTA agency • Attempt to arrive at two economic indicators: ICER, budget impact • Cost-effectiveness linked to explicit or implicit threshold • Supported by structured review • Similaritywith regulatory approaches • Mainly qualitative methodologies based on collective decision-making • No attempt to arrive at ICER: scoring is often used, classification is a priority • Consideration of non-financial aspects & broader societal impact • Synergiesbetween economic evaluation and qualitative assessment • Mainly collective decision-making, which is retraceable and publicly accessible • Cost-effectiveness is one input to a classification /scoring algorithm • Wide consideration of non-financial aspects & broader societal impact TW F I J CAN AUS CH S PL HU UK KS
Cost-effectivenessasthecornerstone of economicevaluation • Cost-effectivenessmeansthat • thenewdrugdeliverslargerhealthbenefitat a lowercostoratthesamecost(‘dominantcase’: therapies ‘B’ and ‘C’ comparedtotherapy‘A’), • thenewdrugcosts more thanthecomparatorbuttheincrementalhealthbenefit is more thantheincrementalcostsincurred(therapy ‘D’ comparedtotherapy ‘A’), • thenewdrugdeliverslowerhealthbenefitcomparedtothecomparator, butthelossinhealthbenefit is lowerthanthedecreaseincosts(notpreferred, therapy ‘K’ comparedtotherapy ‘A’). Health gain (u) Cost of therapy (c)
Economicevaluation – is itreallyabletocapturevalue? Methodologyoverload Lack of pragmatism, mismatchwithhigher-leveldecision-makers’ style Pseudo-objectivity Costly and requirescapabilitieswhicharenon-existentin MIC Perverted incentives, pricingeffect Consultancy business PUBLIC BACKLASH & SHIFT AWAY FROM ONE-SIDED ECONOMIC EVALUATION
Overview of qualitativevalueassessmentcriteriausedincurrentinternationalpractice Source: owncompilation, Jasmine Pwu (Taiwan), JeremyLim (Singapore) Differentsystemsweighelementsdifferently, and no systemcoversallelements. Focusis sometimesmissing. Assessmentcriteriausedindifferentcountriesmaycoversimilarconceptsunderdifferentterminology.
Pragmaticframeworkfor a redundancy-free, balanced system • Unmet need (urgency) Cost-effectiveness Therapeutic value added Therapeutic value added • More favourable side effect profile • Stronger adherence to treatment Szöveg • Higher effectiveness (degree of response) Budget impact Explicit local policy priorities • Cost-effectiveness is necessary but not sufficientfordrugreimbursement • Therapeutic value added is measured along4 factors • Health policy priorities help decide between therapy areas Source: owncompilation
Institutionalbackgroundinmiddle-incomecountries • Severalpayers, complex decision-making processes • Intuitive, rather than analytical, decision-makers at political levels • Budget impact focus, emphasis on financial aspects • Questions aroundthepracticalapplicability of economic evaluation • CAPABILITY GAP, „institutional cost-effiency” Rationalfree-riding: Peeringonselectedinternationalassessment Simplified local evaluation: Veryfocused, pragmatic local assessment Regionalshared service centresforvalueassessment?
Overview of otherstrategicvariablesinmiddle-incomecountries A PARADIGM Economic evaluation Qualitative assessment Balanced assessment B RESOURCELEVEL Heavy model Light model Ultra-light model C SCOPE Only pharmaceuticals Pharmaceuticals, diagnostics and medical devices All health technologies, incl. public health programmes PROCESS AND ORGANIZATION D Independent Drug Committee and HTA Institute Separate department within sick fund (Health Insurance House) Separate department within Ministry of Health PERSPECTIVE E Societal perspective Patient perspective Payer perspective with societal considerations
Qualitative drug assessment Simplified economic evaluation Blueprintprocessforreimbursementdecision-makinginmiddle-incomecountries Technical inspection of dossier PAYER Balancedassessment HTA INSTITUTE First consultation with the manufacturer, discussion of cost- or risk-sharing proposal Drug Committee opinion on cost-effectiveness DRUG COMMITTEE • Second consultation with the manufacturer, renegotiation of cost- or risk-sharing proposal Drug Committee decision on reimbursability Publication of decision, notification of the manufacturer and the payer Signature of cost- or risk-sharing agreement PAYER Listing (adoption to the formulary)
Standardized retraceable decision-making processes with clear milestones and deadlines Pre-defined decision criteria, publicly accessible, intelligible (plainlanguage) individual opinions and collective decisions Full disclosure of eventual conflicting interests Balanced composition and properly designed voting mechanisms of the Drug Committee Individual financial independency of participating experts (remuneration based on agency / ‚national bank model’) Importantproceduralrequirementsfor a balanceddrugassessmentsystem
Recommendedstrategicoptionsfor Romania PARADIGM A Balanced assessment As negative case studies show, HTA implementation based on balanced assessment offers a one-time historic opportunity to bypass practical problems with economic evaluation and the resulting disappointment. B RESOURCELEVEL Ultra-light model As a country with limited financial resources, Romania cannot realistically implement a heavy model, while the light model may have higher cost than benefits. Therefore an ultra-light model may be a rational first step. C SCOPE Only pharmaceuticals HTA for pharmaceuticals carries considerable advantages over other health technologies as methodologies are widely available, and interests and incentives are easier toidentify. D ORGANIZATION Independent Drug Committee and HTA institute Independent Drug Committee and HTA institute can best support retraceable, publicly accessible and intelligible decision-making based on collective reason. PERSPECTIVE E Payer perspective with societal considerations As the goal of HTA is to support reimbursement decisions taken by the payer, the payer’s perspective has to be used, complemented by the analysis of wider societal impact.
Somehigh-levelconclusions There is considerablevariationin HTA systemsallaroundtheworld, withtendenciestowardbalancedassessmentframeworks. Economicevaluation has challengesinmiddle-incomecountries. FollowingthetrackwhichPoland and Hungary has followedinthepastfewyearsis notnecessarilyhelpful. Both theframework and theprocessarecrucial.