Download
1 / 102
2.45k likes | 9.57k Vues
Sella turcica and parasellar region. Zulmarie Roig, MD NSMC, Chief of MRI Department of Radiology. Topics for discussion. Anatomy and variants of the sella turcica and parasellar region Sella turcica and suprasellar region / pathology Parasellar region / pathology

E N D
Sella turcica and parasellar region Zulmarie Roig, MD NSMC, Chief of MRI Department of Radiology
Topics for discussion • Anatomy and variants of the sella turcica and parasellar region • Sella turcica and suprasellar region / pathology • Parasellar region / pathology • Infrasellar and skull base lesions
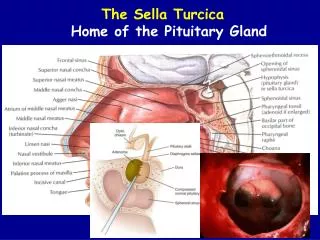
Anatomy of the sella turcica Chiasmatic sulcus Planum sphenoidal Anterior clinoid process Posterior clinoid process Tuberculum sella Dorsum sella Sphenoid sinus Clivus
Sella • Optic canal • Superior orbital fissure • Anterior clinoid process • Foramen rotundum • Carotid sulcus • Foramen ovale • Foramen spinosum • Clivus • Foramen lacerum • Dorsum sellae • Posterior clinoid process • Pituitary fossa • Tuberculum sellae • Chiasmatic recess • Planum sphenoidal • Middle clinoid • Cribriform plate • Middle cranial fossa • Greater wing of the sphenoid Atlas of Neuroradiologic Embriology, Anatomy, and Variants, J Randy Jinkins, 2000, p417, Fig 3-2
Sella turcica size(6 to 21 years) • 5 - 16 mm in anteroposterior diameter • 4 - 16 mm in vertical depth • Accepted normal maximum dimensions of 16 mm in anteroposterior dimension and 12 mm in depth.
Pituitary gland • Anterior lobe • Intermediate lobe • Posterior lobe
Pituitary gland Third ventricle Optic chiasm Medial eminence Anterior lobe Posterior lobe Pars tuberalis Infundibulum Pars distalis Pars nervosa Pars intermedia
Figure 1. Normal sagittal anatomy. Unenhanced sagittal image shows the optic chiasm (C) in the suprasellar cistern, infundibulum (arrowhead), anterior (A) and posterior (P) lobes of the pituitary gland, sphenoid sinus (*)
Pituitary gland • Anterior lobe- intense homogeneous enhancement ( high vascularity and lack of blood brain barrier) • Mild T1 hyperintensity (newborns, pregnant or lactating women) • GH, TSH, ACTH, FSH, LH, prolactin • Intermediate lobe- hypointense (avascular) on post contrast images • MSH • Posterior lobe- Intrinsic T1 hyperintense (90 % of patients, due to antidiuretic hormone neurosecretory granules) • Vasopressin, oxytocin Neuroimaging Clin N Am 15 (2005) 203-219a Radiographics 2006; 26:93-113
Pituitary gland • Shape • Concave superior surface • Convex, or flat- children < 2 years • Height • Children 4-6 mm • Male 6-8 mm • Female 8 mm (up to 10 mm), • Pregnancy 10 mm • Postpartum 12 mm • Gradual decreased in size with age Neuroimaging Clin N Am 15 (2005) 203-219a Radiographics 2006; 26:93-113 AJNR 16:1413-1419, Aug 1995
Pituitary stalk • Lacks BBB- contrast enhancement • Smoothly tapering contour • Transverse diameter • At optic chiasm- 3.25 mm +/- 0.56 • At the insertion- 1.91 mm +/- 0.40 AJR: 159, 375-377,August 1992
Fig. 1.-Ti-weighted (5E 400/12) contrast enhanced coronal MR image of pituitary stalk at level of optic chiasm. Cursor shows how measurements were made in transverse plane. Fig. 2.-Ti-weighted (5E 400/20) contrast enhanced sagittal MR image shows smooth tapering of pituitary stalk. Note comparable enhancement of stalk, tuber cinereum, and median eminence and low signal of central infundibular recess (arrow). AJR: 159, 375-377,August 1992
Sella turcica and pituitary gland variants • Lateral bridge- bony bridge between anterior and posterior clinoid processes • Anterior bridge- bony bridge between anterior and middle clinoid processes • Aplastic or hypoplastic • Duplicated • Intrasellar bony spike • Enlarged, partially empty sella • Predisposed by deficiency of diaphragm sella (roof of pituitary fossa)
Sella turcica and pituitary gland variants • Pituitary gland hypoplasia, hyperplasia, ectopia • Deviation of infundibulum (46 % normal patients) • Optic chiasm is fixed anterior over the tuberculum sellae (5-15%), Neuroimaging Clin N Am 15 (2005) 203-219a
Intrasellar lesions • Adenomas • Apoplexy • Rathke’s cleft cyst • Craniopharyngioma • Meningioma • Pituitary hyperplasia • Aneurysm • Arachnoid cyst • Dermoid/epidermoid • Chordoma
Pituitary adenoma • Macroadenoma (>10 mm) • Comprise 10-15 % all intracranial neoplasm • 1/3-1/2 of the sellar and parasellar masses • Prolactin-constitute 20% of pituitary cells (men and nulliparus women) • Slow growing • Nonsecretory- 60% patient’s with visual deficits • Extend into the suprasellar cistern, cavernous sinuses, sphenoid sinus
Pituitary adenoma • CT • Isointense to brain • Enhance • MR • Isointense to gray matter on T1/T2 • Intense contrast enhancement • Areas of necrosis, hemorrhage • Asymmetric tentorial enhancement – may reflect cavernous vascular congestion or tumor invasion, AJNR 22:1528-1533, Sep 2001
Pituitary adenoma • Microadenoma (<10 mm) • Low area of hypointensity, decreased or non-enhancement • Secondary signs • Depression of the sellar floor • Loss of normal concavity of the superior surface • Displacement of the infundibulum • Peak enhancement –later than the normal gland Endocrinology and Metabolism Clinics of North America, Vol 28 (1), 1999
Figure 3. Time intensity curve comparing the enhancement characteristics of normal pituitary gland with that of a microadenoma. Note the normal gland takes up contrast more rapidly than adenoma tissue and soon begins to wash out. The adenoma curve shows a slower uptake, lower peak enhancement level and prolonged retention of contrast. At time tx the intensity of a microadenoma may equal that of normal gland, potentially obscuring its presence
Figure 4. Coronal dynamic gadolinium enhanced MRI scan demonstrating superior temporal resolution of contrast enhancement in the normal gland surrounding a hypointense microadenoma in the right lobe. Each scan (A-C) was obtained at the same coronal location at one second intervals following IV contrast administration. Coronal unenhanced (D) and delayed enhanced (E) images of the same patient show the microadenoma in the right lobe of the gland (arrow) that is hypointense relative the the normal pituitary tissue.
Pituitary Apoplexy • Acute ischemia and subsequent hemorrhage, necrosis- lack of arterial supply (hypophyseal portal system). • Headache, vomiting, visual loss • Adenomas are prone to hemorrhage and necrosis (large blood supply) • Most common in macroadenomas (20 % of adenomas have hemorrhage) • 25% patients with intratumoral hemorrhage have apoplexy Radiographics 2006; 26:93-113
Pituitary Apoplexy • MR • T1 heterogeneous predominantly T1 hyperintense, T2 predominantly hypointense • Fluid-fluid level • Sheehan’s Syndrome- post partum pituitary hemorrhage secondary to hypovolemia and shock.
Hemorrhage within macroadenoma
Rathke’s cleft cyst • Derived from remnants of Rathke’s pouch- • evagination of primitive oral cavity ectoderm • Extends dorsally and inferiorly to develop into the adenohypophysis • Rare, asymptomatic • Small, intrasellar, and noninvasive • Calcifications-rare, Hemorrhage-extremely rare • Serous or mucoid material, intracystic nodules AJNR 21:485-488, March 2000 • MR • TI hyperintese, T2 hypointense, nonenhancing Radiographics 2006; 26:93-113 Neuroimaging Clin N Am 15 (2005) 203-219a
Meningioma • 15% of intracranial tumors • 5-10% occur in the sellar region • Arise from suprasellar, parasellar, and intrasellar regions • Intrasellar • Rare • Originate from diaphragm sellae • Imaging characteristics • T1 isointense, T2 variable • Homogeneously solid (necrosis, cyst, calcifications occur rarely) • Obtuse dural margins • CSF clefts • Hyperostosis
Sellar metastatic Colon CA
Pituitary Abscess • Rare • Pituitary insufficiency, headache, visual symptoms • Fever, meningitis- infrequent • History- previous surgery • MR • Cystic mass (TI hypointense, T2/FLAIR hyperintense) • Peripheral enhancement, nodular • Bony erosions Turk J Med Sci, 34(2004); 337-339
Suprasellar region • Above the diaphragm sellae • Contains • Optic chiasm • Optic nerves • Infundibulum • Circle of Willis (ACA, BA tip, ACOM, PCOM) • Third ventricle • Hypothalamus, Mamillary bodies
Suprasellar lesions • Extension of pituitary adenomas • Craniopharyngioma • Meningioma • Lymphocytic adenohypophysitis • Metastasis • Chiasmatic/hypothalamic glioma • Lymphoma • Lipoma • Harmatoma • Granuloma/Abscess • Cysticercosis/echinochoccal cyst
Craniopharyngioma • Derived from from Rathke’s pouch • Benign neoplasm • Larger than Rathke’s cleft cysts. Are invasive, and recur. • Suprasellar, can extend into the sella • Bimodal presentation • 5-15 years and 4th to 5th decade