Download
1 / 24
240 likes | 353 Vues
CALGB 90401: A randomized double-blind placebo controlled phase III trial comparing docetaxel, prednisone and placebo with docetaxel, prednisone and bevacizumab in men with metastatic castrate resistant prostate cancer (mCRPC).

E N D
CALGB 90401: A randomized double-blind placebo controlled phase III trial comparing docetaxel, prednisone and placebo with docetaxel, prednisone and bevacizumab in men with metastatic castrate resistant prostate cancer (mCRPC). Wm. Kevin Kelly, Susan Halabi, Michael Carducci, Daniel George, John F. Mahoney, Walter M. Stadler, Michael Morris, Philip Kantoff, Paul Monk, Eric J. Small for the Cancer and Leukemia Group B (CALGB) and Eastern Cooperative Oncology Group (ECOG)
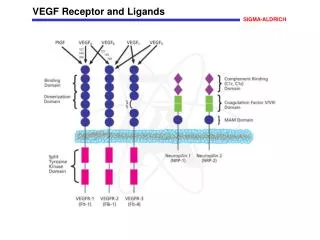
Role of Vascular Endothelial Growth Factor (VEGF) in CRPC Multivariate model of plasma VEGF levels predicting survival time among 197 CRPC patients (George DJ, et al. Clin Cancer Res. 2001 7:1932-6) Lower baseline urinary VEGF levels are associated with improved survival (P = 0.024). (Bok, R. A. et al. Cancer Res 2001;61:2533-2536)
Cancer and Leukemia Group B:Phase II Studies in CRPC 1J Clin Oncol. 2001 May 1;19(9):2509-16 2Cancer. 2003 Dec 15;98(12):2592-8 3Picus et al. Cancer in press
CALGB 90401 • Primary Objective • To determine if the addition of bevacizumab to docetaxel and prednisone increases overall survival compared to docetaxel and prednisone alone in patients with CRPC. • Secondary Objectives • To compare the PFS of these two regimens in patients with CRPC. • To compare the proportion of patients who experience 50% post-therapy PSA decline from baseline. • To compare proportion of patients who have grade 3 or higher toxicities
CALGB 90401: Eligibility Criteria • Progressive adenocarcinoma of the prostate by consensus criteria • No prior cytotoxic chemotherapy or anti- angiogenic agents • Four or more weeks since major surgery or radiation therapy • Eight or more weeks from radio-isotope therapy • ECOG performance status of 0-2 • Signed Informed Consent • Patient with HTN were to be well controlled (< 160/90) • No significant history of bleeding within 6 months of registration • No GI perforation or arterial thrombotic event within 12 months of registration
CALGB 90401: Eligibility Criteria • Required initial laboratory values: • Absolute neutrophil count: ≥ 1500/ µL • Platelet count ≥ 100,000/ µL • Creatinine ≤ 1.5 x ULN • Bilirubin* ≤ 1.5 x ULN • AST ≤ 1.5 x ULN • PSA ≥ 5 ng/ml (non-measurable ds.) • UPC ratio < 1.0 • Serum Testosterone ≤ 50 ng/dl • *Patient with Gilbert’s Disease, ≤ 2.5 x ULN is allowed
CALGB 90401: Stratification Factors • Predicted 24 month survival probability using the nomogram developed by Halabi et al*. • Group 1: < 10% • Group 2: 10-29.9% • Group 3: ≥ 30% • Age • < 65 years • ≥ 65 years • Prior history of arterial events (cardiac ischemia/infarction, cerebral ischemia, peripheral arterial ischemia or CNS hemorrhage. • Yes • No *Halabi et al JCO.2:1232-7, 2003
CALGB 90410: Treatment Schema Arm 1 Dexamethasone 8 mg po x 3 doses Docetaxel 75 mg/m2 on day 1 q 21 days Prednisone 10 mg po daily Bevacizumab1 15 mg/kg IV on day 1 q 21 days RANDOMIZE (1:1) Arm 2 Dexamethasone 8 mg po x 3 doses Docetaxel 75 mg/m2 on day 1 q 21 days Prednisone 10 mg po daily Placebo1 IV on day 1 q 21 days • ASA 325 mg encouraged in all patients that can tolerate • 1In the event of intolerable toxicity to Docetaxel the Bevacizumab\placebo may be continued alone until POD
CALGB 90410: Study Evaluation *Every 3 months until evidence of progression or relapse for a maximum of 5 years from the time of registration
CALGB 90401:Trial Design and Data Analysis • Primary endpoint: Overall Survival (OS) • Secondary endpoint: • 50% decline in PSA1 • Progression Free Survival (PFS)1 • Toxicity • 1050 men randomized • 86% power to detect a hazard ratio (HR) of 1.26 (assume an increase in median OS from 19 mo. in DP to 24 mo. with DP+B) • Final analysis was based on 748 deaths • Primary analysis an intent-to-treat approach using the stratified log-rank statistic adjusting for the stratification factors • Trial was monitored for efficacy and safety by the CALGB DSMB 1PSAWG Criteria, J.Clin.Oncol. 22:537-556, 2004
Median Number of Treatment Cycles Range (0-40) (0-40) (0-40) (0-40) (0-38) (0-37)
Median DP = 21.5 (20.0-23.0) Median DPB=22.6 (21.1-24.5) HR= 0.91 (0.78-1.05)
Median DP = 7.5 (6.7-8.0) Median DPB=9.9 (9.1-10.6) HR= 0.77 (0.68-0.88)
Secondary Endpoints: Objective Response and 50% Decline in PSA
Median Survival (months) Variable HR p-value ARM 1 DP +B Arm 2 DP PS 0.832 0 26.7 23.8 0.081 1 16.7 17.2 0.996 0.971 HGB <=12.8 19.3 17.0 0.815 0.04 >12.8 26.7 26.7 1.045 0.145 ALK <=118 27.9 26.6 1.014 0.902 >118 19.7 16.3 0.02 0.793 LDH <=205 26.0 26.5 1.019 0.87 >205 19.4 16.3 0.802 0.029 PSA <=85 26.6 24.5 0.896 0.323 >85 20.1 18.4 0.892 0.267 TEST <=20 22.6 19.9 0.789 0.016 >20 22.8 1.074 0.549 23.4 Total 22.6 21.5 0.906 0.181 N = 1050 0 0.25 0.5 0.75 1 1.25 1.5 1.75 2 DP better DP + B better Forest Plot of Overall Survival in Select Subgroups
Median Survival (months) Variable HR p-value ARM 1 DP +B Arm 2 DP PS 0.832 0 26.7 23.8 0.081 1 16.7 17.2 0.996 0.971 HGB <=12.8 19.3 17.0 0.815 0.04 >12.8 26.7 26.7 1.045 0.145 ALK <=118 27.9 26.6 1.014 0.902 >118 19.7 16.3 0.02 0.793 LDH <=205 26.0 26.5 1.019 0.87 >205 19.4 16.3 0.802 0.029 PSA <=85 26.6 24.5 0.896 0.323 >85 20.1 18.4 0.892 0.267 TEST <=20 22.6 19.9 0.789 0.016 >20 22.8 1.074 0.549 23.4 Total 22.6 21.5 0.906 0.181 N = 1050 0 0.25 0.5 0.75 1 1.25 1.5 1.75 2 DP better DP + B better Forest Plot of Overall Survival in Select Subgroups
Adverse Events Summary * Infection major cause of treatment related deaths
Conclusions • The addition of bevacizumab to docetaxel/prednisone did not significantly prolong survival in men with metastatic CRPC, although a trend towards improved survival was observed (22.6 vs 21.5 m, p = 0.18). • The addition of bevacizumab to docetaxel/prednisone DID have a significant impact on: PFS 9.9 mo. vs. 7.5 mo. p < 0.0001 Objective RR 53.2% vs. 42.1% p= 0.0113 PSA decline ≥ 50% 69.5% vs. 57.9% p= 0.0002
Conclusions • OS with docetaxel/prednisone is longer than previously reported (21.5 mos vs 19.2 mos in TAX327) and may be due to: • Stage migration • A good risk population (47% of pts had a 24 mo predicted survival of > 30%) • Discrepancy between OS and other markers of clinical benefit such as PFS and RR may be due to: • Impact of longer-than-expected survival in the control group on power calculations • Impact of subsequent therapy on OS • True disconnect between PFS/RR and OS Discordance between OS and PFS\overall response
Conclusions • The addition of bevacizumab to docetaxel/prednisone resulted in more severe toxicities. • The role of anti-angiogenic therapeutics in metastatic CRPC remains to be defined. • Exploratory analysis of patient subsets that may have a clinical benefit from bevacizumab are underway.
Acknowledgements • Patients and families that participated in the study • All colleagues and investigators that contributed to the success of CALGB 90401. • Cancer and Leukemia Group B central office and statistical staff • Eleanor Leung, Ellen Kaplan, Jennifer Williams, John Taylor