Download
1 / 28
290 likes | 416 Vues
“If things were simple, word would have gotten round.” Derrida - 1988. GP4 – Masterclass November 2002 Dr Alan Hassey. Clinical Freedom & Clinical Governance. The freedom to get things wrong? The freedom to do things badly? The freedom to act against patients’ best interests?

E N D
“If things were simple, word would have gotten round.”Derrida - 1988 GP4 – Masterclass November 2002 Dr Alan Hassey
Clinical Freedom & Clinical Governance • The freedom to get things wrong? • The freedom to do things badly? • The freedom to act against patients’ best interests? • The freedom to evade clinical & professional responsibility? • The freedom to offer second-rate care?
How we make decisions • Actuarial judgement is frequently better than clinical judgement • We are better at identifying & coding clinical data than we are at integrating and using it… • We are poor at estimating probabilities - we use heuristics which are generally useful but can lead to systematic errors & biases
How we should make decisions • Application of probabilistic methods to clinical reasoning • Bayesian approach - modify our beliefs in the light of new evidence • Post test P = Pre test P x LR • What place for intuition? • Coping with complexity?
Clinical reasoning, decision analysis & support • Two main themes • The application of appropriate linear, probabilistic models to clinical reasoning • The application of expert judgement to clinical reasoning • Decision Support s/w can apply both statistical and expert judgement systems to the process of clinical care
But we don’t use DS software! • Eccles et al (BMJ link) • No effect was found of computerised evidence-based guidelines on the management of asthma or angina in adults in primary care • There remains the challenge of integrating the systems into clinical encounters where busy practitioners manage patients with complex, multiple conditions
So why health informatics? • Health informatics comprises the science of information management in health care and its application to support clinical practice, decision-making and research. • Triadic consultation • To bring the patient, doctor and relevant information together in such a way as to facilitate clinical care...
The changing consultation • Medieval > pastoralism • Renaissance > EBM (clinical epidemiology) • New world > information age • For health professionals • For patients (as informed consumers) (after Purves)
Within the consultation “The task of the patient is to convey his health beliefs to the clinician; and of the clinician to enable this to happen. The task of the clinician… is to convey her (professionally informed) health beliefs to the patient; and of the patient, to entertain these. The intention is to assist the patient to make as informed a choice as possible about diagnosis and treatment, about benefit and risk and to take full part in the therapeutic alliance”
A cognitive dilemma Need to develop a new intellectual model to weave together these three strands: • The appropriate application of a scientific (probabilistic/linear) method & cognitive model - the traditional scientific clinical method. • The various narratives that make up the patient's health (illness) story • The unpredictable, intuitive, (Balint-like) flash of understanding (non-linear)
Hamm’s Cognitive Continuum • Formal deductive logic/experiment • Controlled trial with explicit degrees of uncertainty • Critical analysis & epidemiological data • System-aided model based on judgement • Peer-aided review • Intuitive (heuristic) judgement
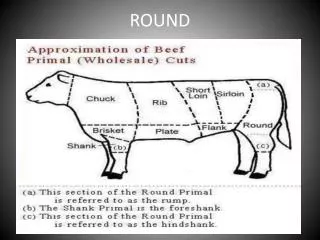
Hospital Higher probability of disease Disease well-differentiated Disease separated from patient Biomedical labelling Diseases stay, patients come & go GP Lower probability of disease Disease poorly-differentiated Patient & illness inseparable No labels in 30% (+) Patients stay, diseases come & go The need for intuitive skills
Complexity • The DPR is a complex system • Some tasks are dealt with better by intuition • Analysis & recording tends to be reductionist (e.g. clinical codes) • Non-linear science allows us to consider narrative & intuition as part of clinical practice
Linear Traditional scientific method Left brain Logical cognitive model Hypothetico-deductive, pattern recognition Probabilistic Reductionist Evidence-based Quantitative Good for complicated problems Non-linear The “art” of medicine Right brain Intuitive cognitive model Interpretive, contextual Unpredictable (within boundaries) Holistic Narrative-based Qualitative Good for complex problems A new model for clinical method
Models in action Need to understand and apply a clinical method that incorporates • Best scientific evidence & cognitive model (alcoholism, poor diet, smoker) • An appreciation of illness narrative (family, sexual & work problems) • A model for the complexity (non-linearity) of the patient’s environment. (Patient as powerless victim, understanding of context)
Promoting intuitive skills • Level 7 of the cognitive continuum? • Suspend analysis • Intuitive mood • Non-judgemental awareness • 90% of communication is non-verbal • Clinician as healer (Balint > doctor as drug)
Decision support • Models • Rule-based (knowledge or probability) • Connectionist (emergent) • Holistic not problem-based • Narrative not codes • Input from non-verbal communication • Annotate & display whole model
General Practice Groupware • Communication • Patient health records for the whole team • Email • Telemedicine • Collaboration • Team guidelines and other knowledge bases • Team-based clinical audit • Computer-based educational resources • Co-ordination • Monitoring the status of actions/tasks • Scheduling resources and tasks
Task model for the clinician in a “simple” consultation • Read the story – viewing the information on computer (pre-consultation), listening, observing, examining and directing conversation • Understanding the story • Utilising the clinical information system (CIS) with the patient • Discussing the options (may involve wider team) • Set therapeutic actions in motion through CIS • Write the story (post-consultation)
Communication Collaboration Co-ordination Links to folk models of health & illness Narrative streams that are patient’s history Coded, H-D or P-R, reductionist model, “doctor-centred” Insight contextual understanding “patient-centred” Doctor as “healer” Family, work & sexual problems Patient Self as “victim”, powerless, enhanced status after OD Alcoholic, smoker, self-neglect, attempted suicide Health interventions – physical, psychological, social Application of EB (Probabilistic) approach to health interventions Links to task models of health & illness