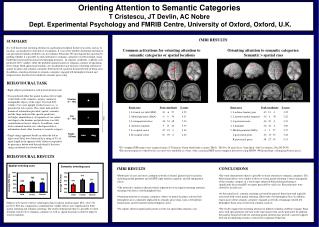
BOLD fMRI
E N D
Presentation Transcript
BOLD fMRI BIAC Graduate fMRI Course September 28, 2004
Why do we need to know physics/physiology of fMRI? • To understand the implications of our results • Interpreting activation extent, timing, etc. • Determining the strength of our conclusions • Exploring new and unexpected findings • To understand limitations of our method • Choosing appropriate experimental design • Combining information across techniques to overcome limitations • To take advantage of new developments • Evaluating others’ approaches to problems • Employing new pulse sequences or protocols
Developments for BOLD MRI • Echoplanar imaging methods • Proposed by Mansfield in 1977 • Ready availability of high-field scanners • Technological developments • Clinical applicability insurance reimbursement clinical prevalence • Discovery of BOLD contrast mechanism
Developments for BOLD MRI • Echoplanar imaging methods • Proposed by Mansfield in 1977 • Ready availability of high-field scanners • Technological developments • Clinical applicability insurance reimbursement clinical prevalence • Discovery of BOLD contrast mechanism
Contrast Agents • Defined: Substances that alter magnetic susceptibility of tissue or blood, leading to changes in MR signal • Affects local magnetic homogeneity: decrease in T2* • Two types • Exogenous: Externally applied, non-biological compounds (e.g., Gd-DTPA) • Endogenous: Internally generated biological compound (e.g., dHb)
External Contrast Agents • Most common are Gadolinium-based compounds introduced into bloodstream • Very large magnetic moments • Do not cross blood-brain barrier • Create field gradients within/around vessels • Reduces T1 values in blood (can help visualize tumor, etc.) • Changes local magnetic fields • Large signal changes: 30-50% • Delay until agent bolus passes through MR imaging volume • Width of response depends on delivery of bolus and vascular filtering • Degree of signal change depends on total blood volume of area • Issues • Potential toxicity of agents (short-term toxicity, long-term accumulation) • Cause headaches, nausea, pain at injection
Belliveau et al., 1990 Slice Location NMR intensity change (CBV) CBV Maps (+24%)
Blood Deoxygenation affects T2 Recovery T2 Decreasing Relaxation Time T1 Increasing Blood Oxygenation Thulborn et al., 1982
Ogawa et al., 1990a • Subjects: 1) Mice and Rats, 2) Test tubes • Equipment: High-field MR (7+ T) • Results 1: • Contrast on gradient-echo images influenced by proportion of oxygen in breathing gas • Increasing oxygen content reduced contrast • No vascular contrast seen on spin-echo images • Results 2: • Examined signal from tubes of oxygenated and deoxygenated blood as measured using gradient-echo and spin-echo images
Gradient Echo Spin Echo ? ? Oxyhemoglobin ? ? Deoxyhemoglobin Ogawa 1990
Gradient Echo Spin Echo Oxyhemoglobin Deoxyhemoglobin Ogawa 1990
Ogawa et al., 1990b 100% O2 Under anesthesia, rats breathing pure oxygen have some BOLD contrast (black lines). Breathing a mix including CO2 results in increased blood flow, in turn increasing blood oxygenation. There is no increased metabolic load (no task). Therefore, BOLD contrast is reduced. 90% O2, 10% CO2
BOLD does not simply reflect blood flow… 0.75% Halothane (BOLD contrast) 3% Halothane (reduced BOLD) 100% N2 (enormous BOLD) Ogawa 1990
BOLD Endogenous Contrast • Blood Oxyenation Level Dependent Contrast • Deoxyhemoglobin is paramagnetic, oxyhemoglobin is less so. • Magnetic susceptibility of blood increases linearly with increasing oxygenation • Oxygen is extracted during passage through capillary bed • Arteries are fully oxygenated • Venous (and capillary) blood has increased proportion of deoxyhemoglobin • Difference between oxy and deoxy states is greater for veins BOLD sensitive to venous changes
MR Signal MR Signal T2 Decay T1 Recovery Effects of TE and TR on T2* Contrast 50 ms 1 s
Kwong et al., 1992 VISUAL MOTOR
Ogawa et al., 1992 • High-field (4T) in humans • Patterned visual stimulation at 10 Hz • Gradient-echo (GRE) pulse sequence used • Surface coil recorded • Significant image intensity changes in visual cortex • Image signal intensity changed with TE change • What form of contrast?
Blamire et al., 1992 This was the first event-related fMRI study. It used both blocks and pulses of visual stimulation. Gray Matter Hemodynamic response to long stimulus durations. White matter Hemodynamic response to short stimulus durations. Outside Head
1. Information processing reflects collected neuronal activity • fMRI response varies with pooled neuronal activity in a brain region • Behavior/cognitive ability determined by pooled activity • Alternatively, if single neurons governed behavior, fMRI activation may be epiphenomenal
BOLD response reflects pooled local field potential activity (Logothetis et al, 2001)
fMRI Hemodynamic Response 1500ms 500ms 100ms Calcarine Sulci Fusiform Gyri
* Calcarine 1500ms 500ms 100ms Fusiform
2. Co-localization • BOLD response reflects activity of neurons that are spatially co-localized • Based on what you know, is this true?
3. Measuring Deoxyhemoglobin • fMRI measurements are of amount of deoxyhemoglobin per voxel • We assume that amount of deoxygenated hemoglobin is predictive of neuronal activity
4. Uncoupling of CBF & CMRO2 • Cerebral Blood Flow (CBF) and Cerebral Metabolic Rate of Oxygen (CMRO2) are coupled under baseline conditions • PET measures CBF well, CMRO2 poorly • fMRI measures CMRO2 well, CBF poorly • CBF about .5 ml/g/min under baseline conditions • Increases to max of about .7-.8 ml/g/min under activation conditions (+ 30%) • CMRO2 only increases slightly with activation • May only increase by 10-15% or less • Note: A large CBF change may be needed to support a small change in CMRO2
Impulse-Response Systems • Impulse: single event that evokes changes in a system • Assumed to be of infinitely short duration • Response: Resulting change in system Impulses Convolution Response = Output
Peak Rise Initial Dip Baseline Undershoot Peak Rise Initial Dip Undershoot Baseline Basic Form of Hemodynamic Response Sustained Response
Baseline Period • Why include a baseline period in epoch? • Corrects for scanner drift across time
Initial Dip (Hypo-oxic Phase) • Transient increase in oxygen consumption, before change in blood flow • Menon et al., 1995; Hu, et al., 1997 • Shown by optical imaging studies • Malonek & Grinvald, 1996 • Smaller amplitude than main BOLD signal • 10% of peak amplitude (e.g., 0.1% signal change) • Potentially more spatially specific • Oxygen utilization may be more closely associated with neuronal activity than perfusion response
Early Evidence for the Initial Dip C A B Menon et al, 1995
Why is the initial dip controversial? • Not seen in most studies • Spatially localized to Minnesota • May require high field • Increasing field strength increases proportion of signal drawn from small vessels • Of small amplitude/SNR; may require more signal • Yacoub and Hu (1999) reported at 1.5T • May be obscured with large voxels or ROI analyses • May be selective for particular cortical regions • Yacoub et al., 2001, report visual and motor activity • Mechanism unknown • Probably represents increase in activity in advance of flow • But could result from flow decrease or volume increase
Subject: 74y male with transient ischemic attack (6m prior) Revealed to have arterial occlusion in left hemisphere Tested in bimanual motor task Found negative bold in LH, earlier than positive in right Negative BOLD response caused by impaired oxygen supply Rother, et al., 2002
Rise (Hyperoxic Phase) • Results from vasodilation of arterioles, resulting in a large increase in cerebral blood flow • Inflection point can be used to index onset of processing
Peak – Overshoot • Over-compensatory response • More pronounced in BOLD signal measures than flow measures • Overshoot found in blocked designs with extended intervals • Signal saturates after ~10s of stimulation
Sustained Response • Blocked design analyses rest upon presence of sustained response • Comparison of sustained activity vs. baseline • Statistically simple, powerful • Problems • Difficulty in identifying magnitude of activation • Little ability to describe form of hemodynamic response • May require detrending of raw time course
Undershoot • Cerebral blood flow more locked to stimuli than cerebral blood volume • Increased blood volume with baseline flow leads to decrease in MR signal • More frequently observed for longer-duration stimuli (>10s) • May not be present for short duration stimuli • May remain for 10s of seconds
Issues in HDR Analysis • Delay in the HDR • Hemodynamic activity lags neuronal activity • Amplitude of the HDR • Variability in the HDR • HDR as a relative measure
Convolving HDR Time-shifted Epochs Introduction of Gaps The Hemodynamic Response Lags Neural Activity Experimental Design
1% 1% Percent Signal Change • Peak / mean(baseline) • Often used as a basic measure of “amount of processing” • Amplitude variable across subjects, age groups, etc. 505 500 205 200
Amplitude of the HDR • Peak signal change dependent on: • Brain region • Task parameters • Voxel size • Field Strength Kwong et al, 1992