Download
1 / 69
690 likes | 1.31k Vues
MANAGEMENT OF Haemorrhoids (piles). Presented by: Dr.Amar P. Dwivedi M.S. ( Ayu .) Ph.D.(Sch.) Associate professor & I/C, Shalya Tantra Dept. Dr.D.Y.Patil Medical ( Ayu .) college, Navi Mumbai Contact number: 09323097013/09757445151 Email: dramar_d@yahoo.co.in

E N D
MANAGEMENT OF Haemorrhoids (piles) Presented by: Dr.Amar P. Dwivedi M.S. (Ayu.) Ph.D.(Sch.) Associate professor & I/C, ShalyaTantra Dept. Dr.D.Y.Patil Medical (Ayu.) college, Navi Mumbai Contact number: 09323097013/09757445151 Email: dramar_d@yahoo.co.in dramar.sarc@gmail.com Website: www.amarayurved.com
Attachments: • Shri Sai Hospital, Thakkar House • Castle Mill Naka,Thane-W • Arogyadham Ayurved Hospital • Manpada, Thane- W • Deerghayu Ayurved Clinic • Devarshi Garden, Majiwada, • Nr. Rutu Park Soc. Thane- W • Aashray Hospital, Gokuleshdham • Sector 5, Ghansoli, Navi Mumbai • Asso.Prof. & In Charge • Shalya Tantra Department • Dr. D.Y.Patil College of Ayurved • & Research Institute, Nerul, • Navi Mumbai
Haemorrhoids Presented by:Dr. Amar P. Dwivedi Profile : • Awarded with: • ‘Aryabhatta Award’, Las Vegas, USA • ‘Dhanvantari Award’, Rajkot, Gujrat • ‘International Excellence Award’, Malaysia • ‘Panacea Excellence Award’, SriLanka • ‘Best Scientific Research Paper ’ winner at • 5th World Ayurved Congress, Bhopal-India & • National Conference-Anusandhan 2010. • Vice President,NIMA- Thane Branch
VARIOUS CONDITIONS IN ANO RECTAL REGION • Imperforate Anus • Piles • Fistula • Fissure • Ischio- rectal Abscess • Proctitis • Enlarged Pappila • Rectal Polyps / Warts • Pilo Nidal sinus • Carcinoma • Pruritis
Any Problem Around The Anus Is Called As.. Piles
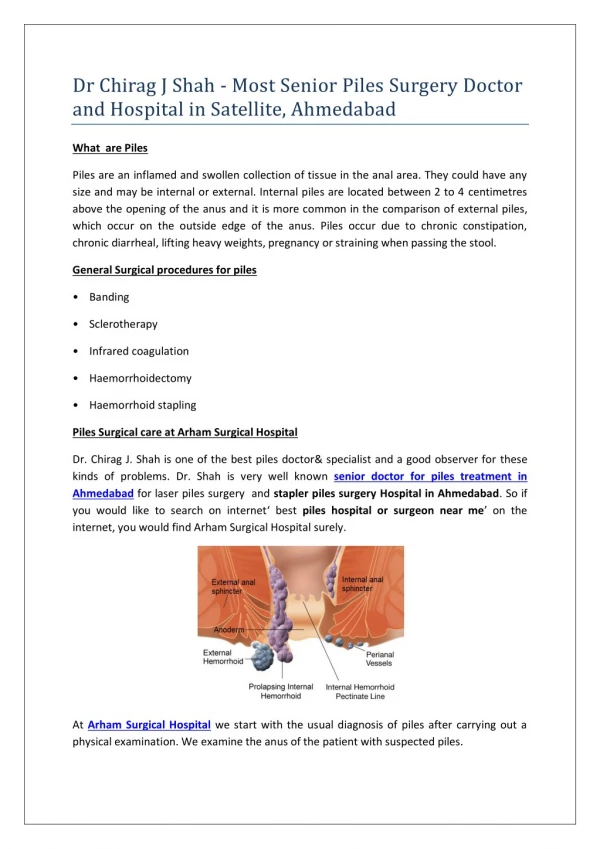
HAEMORROIDS (PILES) Definition : 1.These are the dilated veins within the anal canal in the sub-epithelial region formed by radicals of Superior, Middle and Inferior rectal veins. 2. Piles can be described as masses or clumps ("cushions") of tissue within the anal canal that contain blood vessels and the surrounding, supporting tissue (hemorrhoidal cushions). HaemorrhoidesHaima = blood Roos = flowing Piles Pila = ball Anal cushions : These are submucus venous plexus containing arterial twigs, venules, smooth muscles, elastic tissue & connective tissue. Symptomatic anal cushions are called as piles / haemorrhoides.
INTRODUCTION & INCIDENCE • Humans suffer from piles as a disadvantage of their erect posture. • 50% of people over 50 yrs age suffer from some degree of piles. • 30% of pregnant females suffer from piles • Asymptomatic piles are found in many patients on routine examination • Sex ratio approx. 2M : 1F
TYPES OF HAEMORRHOIDS • According to Symptoms- 1. Bleeding Piles 2. Non Bleeding Piles • According to Origin- 1. Hereditary – Pile mass is present by birth 2. Acquired – Pile mass developed after birth • According to etiology- 1. Primary – Due to indulgence in unsalutary diets & habits 2. Secondary – Due to some other underlying disorders • According to Location- 1. Internal Piles –It is covered with mucous membrane. It arise from Internal Hemorrhoidal plexus & above dentate line. 2. External piles – It is situated outside the anal orifice & is covered by skin. It arise from External Hemorrhoidal plexus & below dentate line 3. Internal + External – Combination variety can also co- exist & is known as Interno- External haemorrhoids.
Degrees of Internal Piles • 3rd-degree • Protrusion outside anal canal at • defecation straining • – needs digital repositioning • 4th-degree • Permanently prolapsed • irreducible piles 1st-degree Projects into anal lumen internally 2nd-degree Protrusion outside anal canal at defecation with spontaneous reduction
Positions of Piles • PRIMARY Right anterior ( 11-o’clock) Right posterior ( 7-o’clock) Left lateral ( 3-o’clock) • Accessory At every o’clock position • DGHAL Arterial cushions at every odd o’clock position i.e. 1 / 3 / 5 / 7/ 9 / 11 o’clock
ETIOLOGICAL FACTORS • Congenital – This is due to ‘ Shukra- Shonitbeejdosh. Pile mass is present by birth. • Anatomical – The haemoroidal veins are situated in anal sub-mucosa in longitudinal direction & does not have support of any other surrounding tissue. So, being valve less structure (either due to any pressure/ obstruction on portal vein or due to gravity) they are always filled with blood which results in its dilatation, elongation & torsion. • Sedentary lifestyle – Long term sitting job, daily traveling • for long distance, engaged in driving or abstinence • from any kind of physical exercise may result in • overfilling in the haemoroidal veins. • Alcohol – Excessive alcohol intake can cause Hepatitis • resulting in portal hypertension which • ultimately exert pressure on the haemoroidal • veins resulting in protrusion of pile pedicle .
Suppression of urge of daefication/ micturation: Suppression of urge of daefication vitiates vat which may result in constipation & further straining while daefication, exerting pressure on the haemoroidal veins. Similarly, frequent IBS or diarrhea may cause mucosal irritation & inflammation resulting in protrusion of pile mass. • Asthma: Asthma or COPD is associated with vigorous & frequent coughing which increases the intra abdominal pressure, thus ultimately exerts pressure on the haemoroidal veins. Similarly, lifting heavy weight can also cause pressure on anal veins. • Enlargement of Prostate: The male suffering from BPH usually strains while micturation & this forceful micturation exerts pressure on the haemoroidal veins. Similarly, patients suffering from urinary calculus & frequent UTI are also prone to such conditions.
Other factors causing Piles: In females- 1) During pregnancy the intra abdominal pressure is increased (due to the foetus) resulting in portal hypertension. 2) At the time of labour (delivery) there is tremendous pressure on the anal canal causing anal fissure and prolapsed piles. 3) Fibroid in uterus may cause pressure on anal veins. Some other factors mentioned in Sushrutsamhita – 1) Straineous work (Balvadvigrah) 2) Anger or sorrowful emotions (Shok) 3) Contradictory food consumption (Adhyashan) 4) Over sex indulgence (Striprasang) 5) Squatting posture (Utkatasan) 6) Horse riding (or long drive) 7) Suppression of natural urge (vegdharan) 8) Diminished Appetite (Mandagni)
Bleeding Swelling / Prolapse Straining / Pain / Discomfort Constipation Itching, Irritation Incomplete evacuation Digital evacuation / instrumentation Abdominal bloating = GAS TROUBLE Lethargy/ Wt. Loss Black-out episodes Symptoms of ANAEMIA SYMPTOMS
Hard stools Straining at defecation Bruising of engorged venous cushions De epithelization Ulceration Bleeding Disruption of sinusoids by straining / irritation Bleeding from pre-sinusoidal arteries Constipation+Straining+IAS spasm Venous back flow Mucosal strech Tear & Bleed Pathogenesis of Bleeding
Bleeding • Occasional to regular / recurrent • Bright red ( from presinusoidal arterial twigs) • Initally Streaks specially with hard stools • Later Steady drip • Advanced Squirts / stream / drip with defecation & Also apart from defecation (blood spotting on undergarments)
Examination • Gain the Confidence of the Patient • Position • Light (Angle- Poise Lamp) • Instruments required like- Gloves, Jelly, Torch, Guaze, Proctoscopes ,Forecep
Position of patient • SIM’S position • Lithotomy position • Knee-Chest position • Prone position
What else is to be kept ready?? • Ears open • Eyes open • MIND open • Gentleness • Respect towards patient • Soft words & politeness • Understanding the patient
What thing to keep away Wicked eyes • Arrogance • Mobile phones • Sharp instruments • Ego Foul thoughts
Inspection • Spread buttocks apart gently • Focus the light source • Observe the peri-anal region & anal verge Skin discoloration Scars, Pruritus, Sinuses, Soiling, Discharge = Pus, Blood etc. External Tag, Swellings (Boil/Induration) ? Sphincter Tone/Spasm (Refluxes) Other Pathologies
Physical examination • INSPECTION: • 1ST-degree = Nil evidence • 2nd-degree = Bogginess at anal verge at affected side, gentle traction on bogginess reveals mucosa • 3rd-degree = Inner red/purplish mucosa & outer skin covered bogginess with linear furrow in between • 4th-degree = Evident irreducible prolapse • White Pannus • Pruritic signs • Soiled perineum
Fissure Hematoma Wart Pilonidal sinus Pruritisani Prolapsed Piles Sentinal pile / tag Bleeding / Discharge External opening of fistula Abscess Sphincter tone Soiling Prolapse during valsalva Stricture / Stenosis Sphincter spasm Worm infestations INSPECTION (Most neglected but most informative)
D.R.E (DIGITAL RECTAL EXAMINATION) P/R examination
Physical examination D.R.E. (Digital Rectal Examination) • Ask patient to bear down & gently insert lubricated gloved finger inside • Early piles = Soft, easily collapsible venous swellings • Late piles = Fibrosis of connective tissue Piles are palpable as soft longitudinal folds Also appreciate : • Anal tone • Ano-rectal sling level • Anal canal length • .Squeeze pressure • Inspect the finger for blood / mucus / feces • Exclusion of other diseases esp. Ca’
Anal Canal Sphincter tone Ano-rectal sling Fibrosis Internal opening of Fistula Induration Tenderness. Rectum Collapsed , ballooned Loaded / empty Wall irregularity & nodularity Stenosis / stricture Polyp / mass Cervix & uterus in females Prostate & seminal vesicles in males Blummer shelf deposits Examine the finger after P/R for blood/mucus/pus/stools P.V. examination with separate gloves PALPATION & DIGITAL RECTAL EXAMINATION (DRE) Peri anal Tenderness, Induration
ANOSCPOY / PROCTOSCOPY • Proper instruments and lighting • Position • Technique • Many things can be diagnosed Physical Examination – With scope inside anal canal, ask patient to bear down & inspect while withdrawing the scope. Look for = bulge – site / covering mucosa colour Bleeding points Rectal mucosa status Other lesions
MANAGEMENT • Acute stage Conservative Treatment: In Allopath,the line of treatment is as follows – 1. In Acute stage i.e. if the patient comes with symptoms like severe pain with haematoma, then Analgesics+ Anti inflammatory + Anaesthetic agent like Xylocaine oint. / jelly is prescribed. Also, patient is asked to take Hot Seitz bath with KMNO4. Haemostatic drugs like Stredron or Ethamsilate can be given to arrest bleeding Generally, the swelling resolves itself. But if the condition do not improved, then it may suppurate or may fibrose giving rise to cutaneous tag or may burst giving rise to bleeding. 2. If haematoma do not resolve, then it is Incised under local anesthesia & the wound is allowed to heal by granulation tissue.
Conservative Management • Diet – Fiber rich, balanced (easy to digest) diet • Ointments - Hydrocortesoneacetate,Heparin sodium, Aminobenzoate,Lignocaine hydrochloride, Zinc oxide • Laxatives - Liquid paraffin, Lactulose, Isabgol, Senna,Castor oil, Bisacodyl • Suppository- Bisacodyl,Glycerene • Analgesics / Antibiotics / Prokinetics • Oral preparations- Sodium picosulphate, Calcium dobesilate, Tranexamic acid • Iron supplement • Seitz’ Bath
Ayurvedic Management Sushruta has mentioned four fold regimen for piles: • Aushadhi Chikitsa i.e Internal medicine effective in I and II grade piles • Kshar chikitsa i.e application of kshar locally or internally effective in I and II grade piles • Agni Karma i.e Excision of pile pedicle by Cauterization • Shalya Karma i.e Ligation and Excision of Pile pedicle effective in III grade and prolapsed pile mass.
Ayurvedic Conservative treatment • Deepan and pachan chikitsa The main objective is to restore the digestive power ( Jatharagni) by: 1. Ajmodadi churna or Hingavasthak churna 2. Chitrakadi or ampachak vati 3. Shankha vati ( form of mild kshar) • Vata anuloman chikitsa For this purpose Avipatikar churna or Panchasakar churna can be prescribed • Mal Sarak chikitsa-(To treat constipation) • Haritaki churna • Abhaya arishta • Triphala churna
To arrest bleeding Nagkeshar Churna, Bolbaddha ras or Kutaj Churna can be given. • Bhalatak kalp in non bleeding piles and kutaj churna • for bleeding piles is choice of drug mentioned in Sushrut. • Various combination for local application • is advocated for initial stage like : • a. Latex of snuhi+ turmeric powder • b. Kasisadi taila • c. Turmeric podwer + Pippli churna+ Gomutra • d. Nimbadi malhara etc.
Specific guidelines mentioned in Sushrut Samhita • In initial stage of piles local application of inform of lep is mentioned which may promote frbrosis and delay the protrusion of pile pedicle • Snuhi latex + Turmeric powder can be tried • Turmeric + Pippali churna + Gomutra can be applied • Specific instruction regarding Diet • Shali, Shasti, Jau or wheat grain mixed with ghrit and milk and gruel is made. This is to taken as diet regularly • Lot of green leafy vegetables • Shatavari mula kalka along with milk • Apamarga mula cooked with rice • Butter milk should be taken regularly after food • Jaggery with haritaki
Kshar Karma in Piles • This is indicated for II Grade internal piles. The kshar is applied to the dilated pile pedicles with the help of specially designed probe known as “Jambaushatha shalaka” under the guidence of proctoscope (Arsho darshan yantra) having slit on its side. • After mild kshar application the pile pedicle is washed with sour gruel (Dhanyaamla) or water and followed by local application of yashtimadu ghrita at the site. • Each pile pedicle is treated differently at the interval of one week. • This may cause fibrosis of the tissues which prevents the pile pedicle from protrusion. Also to some extend it works similar to sclerosing therapy
Use of Kshar sutra in Piles • Some Ayurvedic surgeons prepare a separate kshar sutra which is mild in nature and have less coatings for the ligation of internal pile pedicle. According to them this medicated Kshar sutra simultaneously necroses the pile pedicle, and at the same time they promote fibrosis over the peripheral tissues. • This technique is practiced in few places northern India and is not popular enough. • However this mild kshar sutra can be effectively used in external piles and external sentinel tags.
INJECTION SCLEROTHERAPY HISTORY • = Jhon Morgan of Dublinintroduced this procedure using persulphate of iron • = Mitchell of Clinton-Illionis, USA, used carbolic acid (27–95%) & olive oil HE SOLD THE SECRET TO QUACKS BEFORE HIS DEATH • = Andrews of Chicago, discovered the secret from Quacks and gave it to the world.
Principle of Sclerotherapy Injection of irritant solution evokes inflammatory reaction in submucosa where haemorrhoidal vessels lie. This results in 1) Encasement, which prevents defecatory trauma & thus prevents bleed 2) Blockage of hemorrhoidal vessels, which do not bulge on straining 3) Fibrosis, which fixes mucosa to muscle & prevents prolapse.
INDICATIONS FOR SCLEROTHERAPY • INTERNAL PILES ONLY BEST = for Grade – I, Bleeding Piles GOOD = for Grade – II bleeding piles PALLIATIVE = for Grade – III bleeding piles
Contra – Indications for Sclerotherapy • External Piles • Associated Anal Lesions eg; fissure, fistula, skin tags • Attack of thrombosed internal piles • Pregnancy • Crohn’s / Ulcerative colitis
Phenol Various vegetable oils eg. Almond / olive / coconut STD (sodium tetradecylsulphate) Carbolic acid Sodium morrhuate Quinine & urea hydrochloride Glycerine Polidocanol 5 – 7ml (max = 10 ml) 1 – 2ml Solutions used for Injection: Dosage per pile mass
Site of Injection-In submucosa-Into pile mass - At the pedicle of the pile mass at ano- rectal ring (ALBRIGHT’S method)
Post-procedure Instructions • Mild discomfort • Tenesmus • Follow – up after 3 wks • Watch for fever / pain / bleeding.& inform sos
Advantage of Sclerotherapy • Easily learned procedure • Stops bleeding in 24 - 48 hrs in majority of cases • Cost – effective • Office procedure so early return to work • Painless • Can be repeated
Complications of Sclerotherapy Injection ulcer Paraffinoma • Fainting / Giddiness • Necrosis • Re-Bleed • Abscess • Stricture • Urine retension • Burning & itching • Fistula formation 13/41
Results after Sclerotherapy • Grade – I piles == 98 % • Grade – II piles == 68% • Grade – III piles == 31% • Overall 77% successful • Especially in stopping bleeding • But has less effect on prolapsing element of pile
Principle of RBL • Rubber ring ligature applied to the mucosal covered part of the Internal Pile through a proctoscope • This strangulates the feeding vessel to the pile and gradually cuts through the mucosa • The pile thus sloughs off after 7 – 14days
Indication for RBL • Ideal for Grade – II internal piles • Early Grade -- III internal piles • Contra-indications • Bleeding diathesis (???) • Infection ( fistula / abscess) • Fissure
Post – procedure Instructions • Dull ache / fullness of rectum may be present • Urge to defecatemay be there • Bleeding may occur ----- clots = 1-2days ----- spots = 5 – 14days Follow-up after 2 weeks