Download

1 / 15
0 likes | 11 Vues
Addition of stereotactic radiosurgery (SRS) to molecularly targeted therapies like TKIs in driver mutation-positive non-small cell lung cancer with persistent brain metastases is being investigated in the randomized phase 2 OUTRUN-P trial. The optimal sequencing of SRS and TKIs for NSCLC with brain metastases remains unclear. Ongoing trials are evaluating the effects of SRS combined with continuing TKIs on intracranial disease progression-free survival at 12 months. Eligible patients have received TKIs for 3 months, have up to 10 brain lesions, and are asymptomatic or mildly symptomatic. The primary outcome is intracranial progression-free survival at 12 months. Secondary outcomes include time to local and distant brain failure, salvage therapies, progression-free survival, overall survival, adverse events, and quality of life.

E N D
Addition of stereotactic radiosurgery to molecularly targeted therapies in driver mutation positive non-small cell lung cancer with persistent brain metastases: a randomized phase 2 trial (OUTRUN-P) Yu Yang Soon BSc MBBS MSc FRANZCR National University Cancer Institute, Singapore National University Hospital, Singapore NHMRC Clinical Trials Centre, University of Sydney

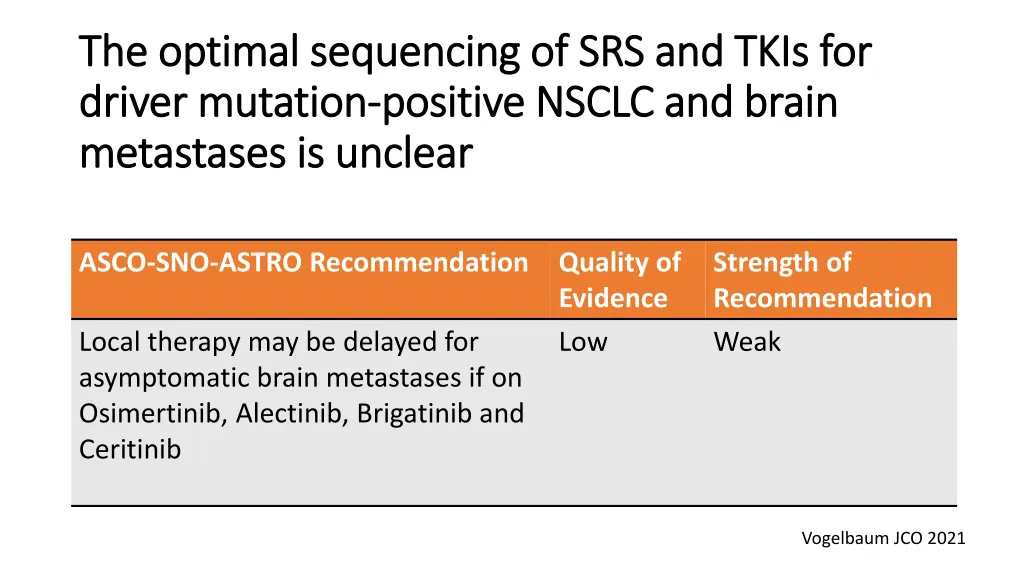
The optimal sequencing of SRS and TKIs for The optimal sequencing of SRS and TKIs for driver mutation driver mutation- -positive NSCLC and brain positive NSCLC and brain metastases is unclear metastases is unclear ASCO-SNO-ASTRO Recommendation Quality of Evidence Low Strength of Recommendation Weak Local therapy may be delayed for asymptomatic brain metastases if on Osimertinib, Alectinib, Brigatinib and Ceritinib Vogelbaum JCO 2021
Is there a role for SRS for EGFR mutant brain metastases Is there a role for SRS for EGFR mutant brain metastases that did not achieve complete response with Osimertinib? that did not achieve complete response with Osimertinib? Stanford Cancer Center Median time: 7 weeks Range: 2 – 18 weeks 239 brain lesions Untreated by RT Asymptomatic No Leptomeningeal disease Median time: 2.5 weeks MRI brain imaging Osimertinib Cumulative incidence of local progression from initiation of Osimertinib Complete response (n = 13) (5%) Partial response (n =197) (82%) Stable disease (n = 29) (12%) 12 months 0% 4% 11% 18 months 0% 6% 17% 24 months 0% 6% 17% 36 months 0% 6% 24% Hui JNO 2022

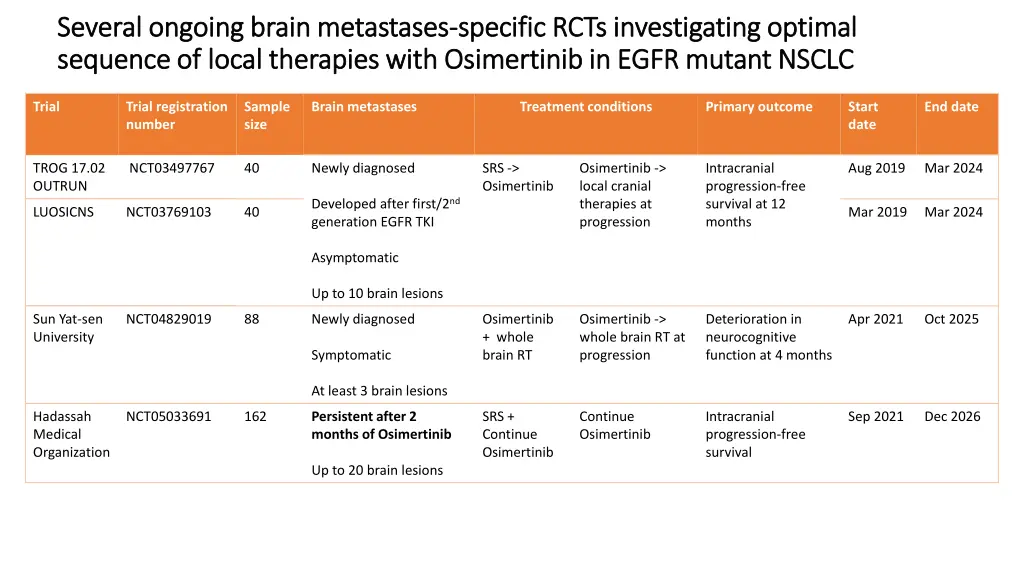
Several ongoing brain metastases Several ongoing brain metastases- -specific RCTs investigating optimal specific RCTs investigating optimal sequence of local therapies with Osimertinib in EGFR mutant NSCLC sequence of local therapies with Osimertinib in EGFR mutant NSCLC Trial Trial registration number Sample size Brain metastases Treatment conditions Primary outcome Start date End date TROG 17.02 OUTRUN NCT03497767 40 Newly diagnosed SRS -> Osimertinib Osimertinib -> local cranial therapies at progression Intracranial progression-free survival at 12 months Aug 2019 Mar 2024 Developed after first/2nd generation EGFR TKI LUOSICNS NCT03769103 40 Mar 2019 Mar 2024 Asymptomatic Up to 10 brain lesions Sun Yat-sen University NCT04829019 88 Newly diagnosed Osimertinib + whole brain RT Osimertinib -> whole brain RT at progression Deterioration in neurocognitive function at 4 months Apr 2021 Oct 2025 Symptomatic At least 3 brain lesions Hadassah Medical Organization NCT05033691 162 Persistent after 2 months of Osimertinib SRS + Continue Osimertinib Continue Osimertinib Intracranial progression-free survival Sep 2021 Dec 2026 Up to 20 brain lesions
Primary Objective Primary Objective To compare the effects of SRS plus continuing tyrosine kinase inhibitors versus continuing tyrosine kinase inhibitors on 12-months intracranial disease progression-free survival in driver mutation-positive NSCLC with persistent brain metastases (up to 10 lesions) after 3 months of tyrosine kinase inhibitors
Eligibility criteria Eligibility criteria 1. Had 3 months of TKIs 2. Up to 10 lesions 3. Asymptomatic or mildly symptomatic 4. At least one lesion amenable to SRS 5. Maximum size of a single lesion is 3cm 6. No Leptomeningeal disease 7. No prior cranial RT Same eligibility criteria for OUTRUN and LUOSICNS

Treatment conditions Treatment conditions Local therapies at progression Continue TKIs + SRS Randomize (1:1) Continue TKIs Local therapies at progression SRS: 15-20Gy in a single fraction depending on the size of the lesion or 24Gy in 3 fractions Osimertinib: 80mg once daily Alectinib: 600mg twice daily Brigatinib: 90mg once daily for 7 days. Increase to 180mg once daily if well tolerated Ceritinib: 450mg once daily

Outcomes Outcomes Primary outcome Intracranial progression-free survival at 12 months Secondary outcomes Intracranial progression-free survival Time to local brain failure Time to distant brain failure Time to salvage local cranial therapies Progression-free survival Overall survival Adverse events Health-related quality of life Same outcomes for OUTRUN and LUOSICNS
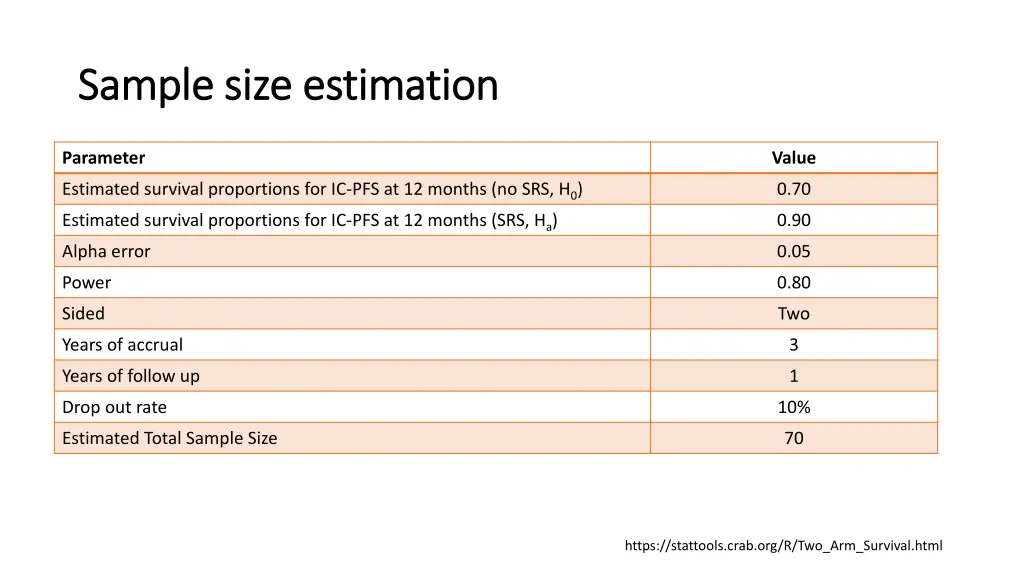
Sample size estimation Sample size estimation Parameter Value Estimated survival proportions for IC-PFS at 12 months (no SRS, H0) Estimated survival proportions for IC-PFS at 12 months (SRS, Ha) Alpha error 0.70 0.90 0.05 Power 0.80 Sided Two Years of accrual 3 Years of follow up 1 Drop out rate 10% Estimated Total Sample Size 70 https://stattools.crab.org/R/Two_Arm_Survival.html
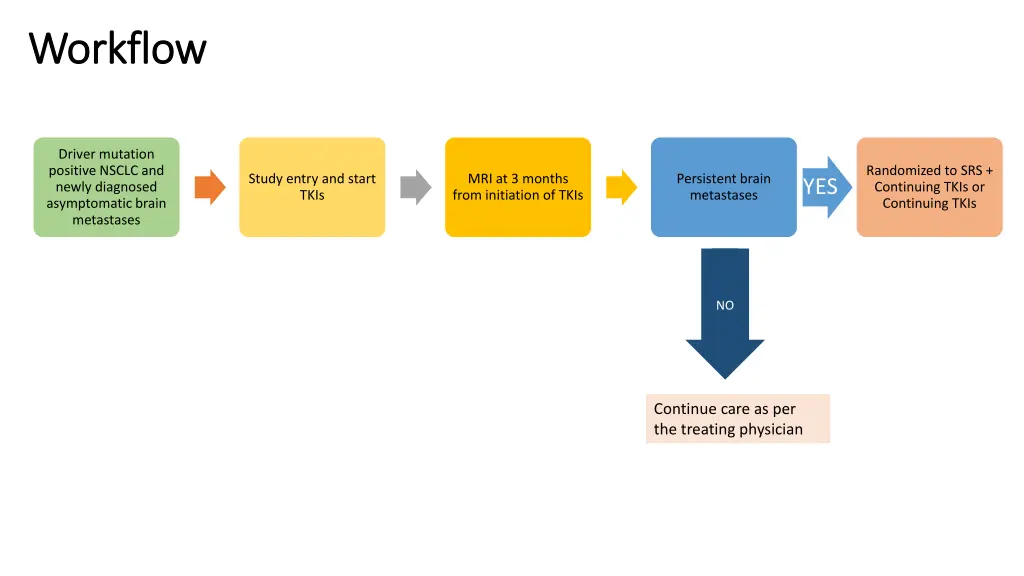
Workflow Workflow Driver mutation positive NSCLC and newly diagnosed asymptomatic brain metastases Randomized to SRS + Continuing TKIs or Continuing TKIs Study entry and start TKIs MRI at 3 months from initiation of TKIs Persistent brain metastases YES NO Continue care as per the treating physician
ASCO ASCO- -SNO Local therapy may be deferred for selected patients with Local therapy may be deferred for selected patients with asymptomatic brain metastases asymptomatic brain metastases SNO- -ASTRO guidelines: ASTRO guidelines: Cancer Types CNS active molecular targeted therapies Quality of Evidence Strength of Recommendation PDL1 positive NSCLC Pembrolizumab + Platinum + Pemetrexed HER2 positive breast cancer, progressed on trastuzumab, pertuzumab and TDM1 Tucatinib + Trastuzumab + Capecitabine LOW WEAK Melanoma (regardless of BRAF) Ipilimumab + Nivolumab Melanoma (BRAF-V600E mutation) Dabrafenib + Trametinib Vogelbaum JCO 2021

This trial concept has the potential to scale up to include other disease types This trial concept has the potential to scale up to include other disease types OUTRUN / LUOSICNS Osimertinib EGFR mutant NSCLC R SRS + Osimertinib Pembrolizumab + Platinum + Pemetrexed Asymptomatic brain metastases PDL1 positive NSCLC R SRS + Pembrolizumab + Platinum + Pemetrexed Tucatinib + Trastuzumab + Capecitabine HER2 positive breast cancer R SRS +Tucatinib + Trastuzumab + Capecitabine

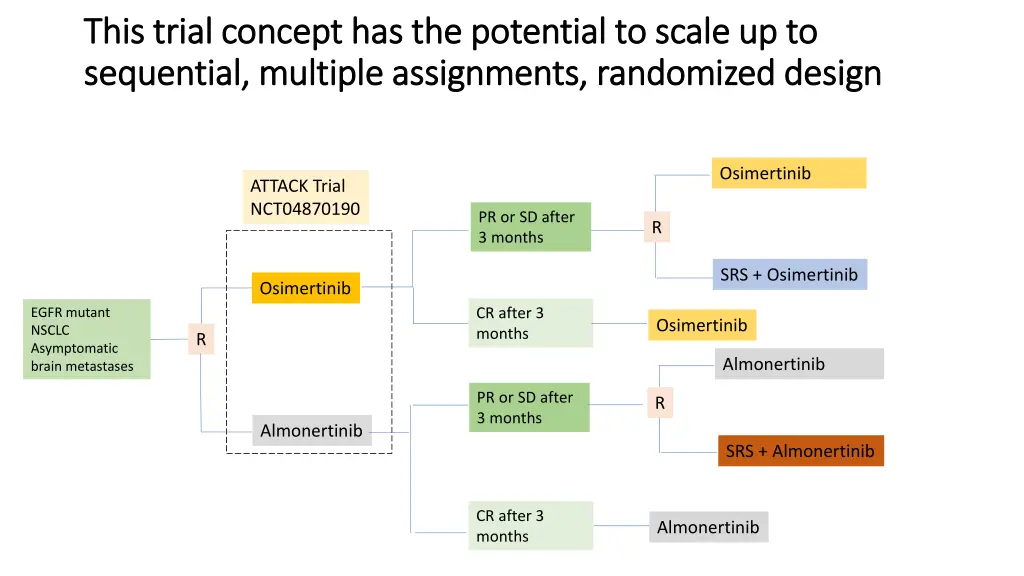
This trial concept has the potential to scale up to This trial concept has the potential to scale up to sequential, multiple assignments, randomized design sequential, multiple assignments, randomized design Osimertinib ATTACK Trial NCT04870190 PR or SD after 3 months R SRS + Osimertinib Osimertinib CR after 3 months EGFR mutant NSCLC Asymptomatic brain metastases Osimertinib R Almonertinib PR or SD after 3 months R Almonertinib SRS + Almonertinib CR after 3 months Almonertinib
Plans on moving this concept forward Plans on moving this concept forward 1. Await readout of OUTRUN and LUOSICNS results 2. Adjust the sample size calculation 3. Engage investigators of OUTRUN and LUOSICNS for support 4. Engage TROG, TOGA and COGNO for support 5. Apply for funding 6. Engage GCCTI team on how to evolve this brain metastases specific RCT to include other disease types and other CNS active molecular targeted therapies
Discussion questions with panel Discussion questions with panel 1. Is there sufficient equipoise for a randomized study? 2. Will patients be interested in participating in this study? 3. Should other newer generations of TKIs be allowed? 4. Should > 10 brain metastases be allowed? 5. How to incorporate translational sub-studies? 6. Other questions?

![[PDF] Free Download Justice on Trial By Mollie Hemingway & Carrie Severino](https://cdn4.slideserve.com/8373939/slide1-dt.jpg)