Download
1 / 66
880 likes | 1.33k Vues
Muscle Contraction and Energy Metabolism. Prof. Dr. Serdar Öztezcan Medical Biochemistry. Contents. structure of muscles mechanism of contraction energy metabolism for contraction similarities and differences in muscles clinical correlation s. Introduction. The largest single tissue

E N D
Muscle Contraction and Energy Metabolism Prof. Dr. Serdar Öztezcan Medical Biochemistry
Contents • structure of muscles • mechanism of contraction • energy metabolism for contraction • similarities and differences in muscles • clinical correlations
Introduction • The largest single tissue • 25% of total body mass in newborn • more than 40% in the young adult • less than 30% in the aged adult
Introduction • Three types of muscle • skeletal • cardiac • smooth
Introduction • Their common function is the conversion of chemical energy to mechanical energy • They differ • mechanism of initiation of contraction • rate of force development • duration of contraction • substrate utilization • innervation • contractile protein arrangement • propagation of depolarization
Introduction • Muscle activity is a major determinant of the overall metabolic rate in both the basal and active state • Loss of muscle mass has a profound effect on overall metabolism • Advancing age and wasting diseases are conditions associated with loss of muscle mass • This loss is associated with increased morbidity and mortality
Introduction • Skeletal muscle • locomotion • a source of body heat • provides amino acids for hepatic gluconeogenesis • major site of glucose and triglyceride disposal
Structure • A common characteristic of cardiac myocytes, smooth muscle cells and skeletal myofibers is that their cytoplasm is packed full of contractile protein • The contractile protein is arranged in linear arrays of sarcomere units in skeletal myofibers and cardiac myocytes..... striated muscle • Contractile protein in smooth muscle cells is not organized into a sarcomeric structure ....... nonstriated muscle
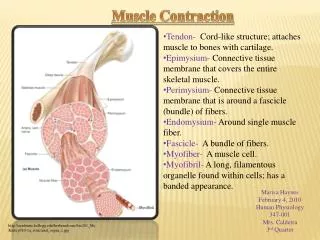
Structure • Skeletal muscle consists of bundles (fasciculi) of elongated, multinucleated fiber cells(myofibers) • surrounded by an excitable plasma membrane sarcolemma • Fiber cell contains a bundle of many myofibrils • embedded in intracellular fluid termed sarcoplasm • Myofibrils are composed of thick and thin myofilament proteins • the thick filament ...... myosin • the thin filament ....... actin, tropomyosin and troponins • form the sarcomere
Structure (Summary) • Microscopic unit, • fasciculus: bundle of muscle cells • Cellular unit, • myofiber: long, multinucleated cell • Subcellular unit • myofibril: composed of myofilament (thick, thin) proteins • Myofilament components • proteins; primarily myosin and actin • Functional unit • sarcomere: repeating unit of the myofibril
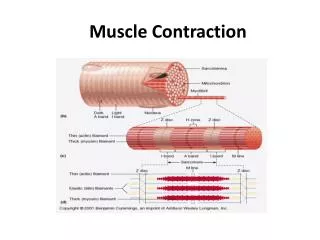
Sarcomere • Electron microscopic analysis of myofibril reveals a repeating pattern of light- and dark-staining regions • These regions are known as the I (isotropic)- and A (anisotropic)-bands, respectively • At the center of the I-band is a discrete, darker staining Z-line • the center of the A-band has a lighter staining H-zone with a central M-line • The sarcomere is centered on the M-line, extending from one Z-line to the next • The M-and Z-lines are base plates for anchoring the filaments
Sarcomere proteins;Myosin • one of the largest proteins in the body • accounts for more than half of muscle protein • primary component of the thick filament • made of two heavy chains and four light chains • heavy chain can be subdivided into the helical tail and globular head regions • light chains are bound to the globular heads • two flexible hinge regions • myosin filaments are associated through their helical regions and extend outward from the M-linetoward the Z-line
Myosin • There are several features of myosin that are essential for muscle contraction • Myosin binds reversibly actin to form actomyosin (actin-myosin) • globular heads have binding sites for ATP and its hydrolysis products, ADP and phosphate (Pi) • globular heads have a Ca2+-dependent ATPase activity
Sarcomere proteins:Actin • composed of G-actin (globular), which polymerize into a filamentous array (F-actin) • Two polymer chains coil around one another to form the F-actin myofilament • F-actin is the major component of the thin filament and interacts with myosin in the actomyosin complex • The F-actin chains extend in opposite directions from the Z-line, overlapping with the myosin
Sarcomere proteins:Tropomyosin and Troponins • Tropomyosin is a fibrous protein that extends along the grooves of F-actin • The troponin complex is bound to tropomyosin: • Tn-T (tropomyosin-binding) • Tn-C (calcium-binding) • Tn-I (inhibitory)
Clinical correlation:Myocardial Infarction • The cardiac troponins differ slightly from those in skeletal muscle • Specificity in clinical diagnostic test for Myocardial Infarctus
THE CONTRACTILE PROCESS The sliding filament model • Based on morphologic observation on resting and contracting muscle • When muscle contracts, there is no change in lengths of the thick and thin filament, but sarcomere, H zone and the I bands shorten
The sliding filament model • In resting, relaxed muscle (1) • calcium concentration is 10-7 mol/L • head of myosin contains bound ADP and Pi • head of myosin is extended from the axis of helix(90o cocked state ) in a high-energy conformation • Although the myosin-ADP-Pi complex has a high affinity for actin, binding of myosin to actin is inhibited by tropomyosin, which blocks the myosin-binding site on actin at low calcium concentration
the sliding filament model (cont) • When muscle is stimulated (2) • calcium enters the sarcoplasm through voltage-gated calcium channels • calcium binding to Tn-C causes a conformational change in Tn-I, which is transmitted through Tn-T to tropomyosin • movement of tropomyosin exposes the myosin-binding site on actin • Myosin-ADP-Pi binds to actin, forming a“cross-bridge”
the sliding filament model (cont.) • power stroke (3) • release of Pi, then ADP from myosin during the interaction with actin is accompanied by a major conformational change in the hinge regionsof myosin • snap back to their original 45oangle with the tails, producing the 'power stroke‘ • moves theattached actin towards M bond • increases their overlap and causing muscle contraction • myosin is now in low-energy state (No ADP- ATP)
the sliding filament model (cont.) • preperation to next (4) • Ca2+ pumped back into sarcoplasmic reticulum by Ca2+-ATPase and Na+/ Ca2+-antiporter • Release of Ca2+ from troponin • binding of ATP to myosin leads to dissociation of the cross-bridge • hydrolysis of ATP restore the high-energy conformation, setting the stage for continued muscle contraction
Rigor Mortis • The increase in Ca2+ in the sarcoplasm and decrease in ATP after death lead to tight binding between myosin and actin, forming rigid muscle tissue
Muscle membrane depolarization : Skeletal muscle • Stimulus leads to depolarization of the electrochemical gradient across the sarcolemma • caused by influx of Na+ • propagates rapidly along the sarcolemma • is transmitted into the muscle fiber by invaginations of the plasma membrane, called transverse tubules (T tubule), • signals a voltage-gated calcium channels • leads to rapid, concerted release of calcium from the sarcoplasmic reticulum (SR), • is rich in a Ca2+-binding protein, calsequestrin
Muscle membrane depolarization : Skeletal muscle • In order for repolarization to occur again, sodium must be actively pumped out of the cytosol by Na+/K+-ATPase pumps • The rate of muscle repolarization is affected by both the rate and density of these pumps • Higher levels of Na+/K+-ATPaseactivity are found in fast contracting muscles • Increased Na+/K+-ATPasepump density is an important adaptation to exercise
MUSCLE ENERGY METABOLISM • Muscle is the major consumer of fuels and ATP in the body • ATP is used for • contractile process • restoration of intracellular calcium levels • maintenance of ion gradients • Three ATPases are required • Myosin-ATPase • Ca2+-ATPase • Na+/K+-ATPase • Decreased ATP availability or inhibition of any of these ATPases will cause a decrease in muscle force production
ATP • The amount of ATP in skeletal muscle is only sufficient for a few seconds, so that ATP must be constantly renewed • Energy systems for muscle contraction • the creatine phosphate shuttle • anaerobic glycolysis (using blood glucose or muscle gycogen) • aerobic metabolism via oxidative phosphorylation • a reaction catalyzed by adenylate kinase (from two molecules of ADP )
Contractions • The energy systems that synthesize ATP are not equivalent, and directly affect the amount and duration of power output from the contracting muscle • There are two main types of contractions • Short-duration, high-power output contractions • Low-intensity, long-duration contractions
Short-duration, high-power output contractions • High force output can only be maintained for a short period of time • Contractions at maximal power levels depend on • high myosin-ATPase • rapid ATP resynthesis by using the high energy compound creatine phosphate • Creatine is synthesized from arginine and glycine and is phosphorylated reversibly to creatine-P by the enzyme creatine (phospho) kinase (CK or CPK) • CK : Creatine + ATP Creatine-P + ADP • MM (skeletal muscle) • BB (brain) • MB (enriched in cardiac tissue)
Short-duration, high-power output contractions (cont.) • The level of creatine-P in resting muscle is several-fold higher than that of ATP • Thus, ATP concentration remains relatively constant during the initial stages of exercise • Creatine phosphate stores decline rapidly during the first minute of high power output muscle contraction • ATP is also replenished by adenylate kinase (myokinase) as follows: • Adenylate kinase: 2ADP ATP + AMP
Clinical correlation:CK and CK-MB • Total CK:Diagnosis muscle disorders • CK-MB : Diagnosis Myocardial Infarction
Clinical correlation:Creatinin • Creatine phosphate is unstable and spontaneously cyclizes to form creatinine, which is excreted in theurine • The spontaneous production of creatinine occurs at a constant rate and isproportional to body muscle mass • Thus, the amount of creatinine excreted eachday (the creatinine clearance rate) is constant and can be used as an indicator ofthe excretory function of the kidneys