Download
1 / 52
520 likes | 781 Vues
Withdrawal Management as a Bridge to Recovery. George Kolodner, M.D. June 2013. Agenda. Welcome and Introduction Pre-Assessment Review Learning Objectives Discuss Withdrawal Management as A Bridge to Recovery Questions & Answers Post-Assessment Evaluations. Learning Objectives .

E N D
Withdrawal Management as a Bridge to Recovery George Kolodner, M.D. June 2013
Agenda • Welcome and Introduction • Pre-Assessment • Review Learning Objectives • Discuss Withdrawal Management as A Bridge to Recovery • Questions & Answers • Post-Assessment • Evaluations
Learning Objectives • At the end of this session you will be able to: • Identify the early signs of alcohol withdrawal • Know the time frames of alcohol, benzodiazepines, opioid, and tobacco withdrawal syndromes • Understand the strategy for the treatment of withdrawal and be familiar with medications used
Uses for Addiction Medication • Withdrawal management: • Benzodiazepines and anticonvulsants for alcohol • Suboxone (buprenorphine) and methadone for opioids • Phenobarbital for benzodiazepines • Chantix (varenicline) for tobacco • Stabilization and maintenance • Suboxone (buprenorphine) and methadone for opioids • Relapse prevention • Antabuse (disulfiram) and Campral (acamprosate) for alcohol • Vivitrol/Revia (naltrexone) for alcohol and opioids • Chantix (varenicline) for tobacco
Withdrawal Management (“WM”) • Withdrawal Management is a set of procedures designed to reduce or eliminate the discomfort and danger from discontinuing the use of substances to which a person has become physically dependent.
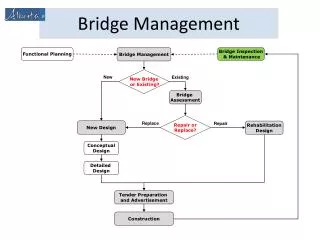
Withdrawal Management at Kolmac • Kolmac Clinic has pioneered in withdrawal management in two ways: • Expanding its use in an ambulatory setting • Combining it with an Intensive Outpatient Program (IOP) rehabilitation to prevent the “revolving door” scenario of repeated readmissions without follow-up treatment
Ambulatory WM/IOP Combination • Primary purpose: To engage the addict in Treatment after withdrawal • Reduces apprehension about structured group program by immediate exposure to group
Kolmac MedicationPreferences(Brand Names are Capitalized) • For alcohol • Librium (chlordiazepoxide) • For benzodiazepines • (phenobarbital) • For opioids • Suboxone (buprenorphine) • For tobacco • Chantix (varenicline)
Ideal Medication • Compared to the addicting drug, it is: • Cross-tolerant • Longer acting • Less toxic • Easily administered • Less reinforcing
What is the Goal? Maximize Comfort
Post-Acute Withdrawal Syndrome (PAWS) PAWS is a set of troublesome symptoms that persist for days to weeks after the acute symptoms have resolved. • Issues • Reassurance and education as a primary intervention • Importance of avoiding iatrogenic cross addiction by delay of medication tapering • Differentiate from re-emergence of co-occurring anxiety disorder
Clinical Relevance of Withdrawal Severity by Drug High • Alcohol • Benzodiazepines • Opioids • Tobacco Low • Marijuana • Perhaps higher for synthetic forms “Spice” None • Ecstasy (MDMA) • Cocaine • Ketamine • Amphetamines • PCP (Phencyclidine)
1. Alcohol Withdrawal Syndrome (AWS):Time Frame After Last Drink • Typical • Begins: 6 to 24 hours • Peaks: at 36 hours • Diminishes: over next 1 to 2 days • Seizures: usually within 8 to 24 hours • Risk increases with: • Repeated withdrawals • Combined with withdrawal from sedatives • Delirium Tremens (“DTs”): appear in 3 to 4 days
Some Factors Making AWS Prediction Difficult Include: • The number of days of daily drinking to create physical dependence has not really been determined • Patients sometimes: • Do not accurately report the time of the last drink • Will minimize a past history of withdrawal symptoms • May be amnestic for their experience will alcohol withdrawal delirium
These problems can be reduced if: • Additional information from collateral sources can be obtained. • Blood alcohol level is measured with breathalyzer.
Alcohol Withdrawal Syndrome The possibility that an AWS will develop must be considered if the patient reports daily heavy drinking -- especially if it begins early in the day – and has not been abstinent in the preceding 48 hours.
AWS: History That Indicates High Risk • High tolerance • Previous history of withdrawal symptoms • Drinking begins shortly after awakening • No history of 24 hours abstinence
AWS: Early Symptoms and Signs • Anxietyis the earliest indication • Ask: “Do you feel nervous when you go a day without drinking?” • Sweating: note sweaty palms • Tremulousness • Initially not visible, but patient “feels shaky” • Becomes visible on movement • Hands with arms extended and fingers spread • Tongue • Progresses to being visible at rest • Insomnia on first night not drinking
Anticonvulsants as an Alternative or Supplement to Benzodiazepines • Rationale • No sedation or ataxia • No abuse potential • For mild to moderate symptoms (CIWA < 15) • Start: Tegretol (carbamazepine) 200 mg • Day 1: Four time daily • Days 2 to 4: Reduce by once daily then stop • Next: Neurontin (gabapentin) 300 mg three times daily for 2 weeks • To reduce post-acute withdrawal symptoms
Tracking Progress of AWS Treatment • Single question: “On a scale of zero to ten, where zero is no withdrawal discomfort and ten is the worst discomfort you have ever had, what number would you put on your withdrawal discomfort right now?” • Repeat the question periodically and try to get patient’s symptoms to zero.
2. Benzodiazepine Withdrawal Syndrome: Issues • For a given individual, the symptoms of withdrawal tend to fluctuate more than do symptoms of alcohol withdrawal • Tremor and measurable signs may not accompany the patient’s symptoms
Benzodiazepine Withdrawal Syndrome: Issues (Continued) • No consensus regarding validated severity scales • The simultaneous re-emergence of underlying anxiety and insomnia can resemble the withdrawal symptoms
Benzodiazepine Withdrawal Syndrome: Time Frame After Last Pill • Short acting (Xanax, Ativan) • Onset: Within 24 hours of cessation • Peak severity: 1 to 5 days • Duration: 7 to 21 days • Long acting (Valium, Klonopin) • Onset: Within 5 days of cessation • Peak severity: 1 to 9 days • Duration: 10 to 28 days
Medicating Benzodiazepine Withdrawal Syndrome - 1 • Medication choices • phenobarbital • Allows urine tracking of benzodiazepine relapse • Useful for double addiction to alcohol and high potency benzodiazepine • Klonopin (clonazepam) • Better for high potency benzodiazepines • Librium (chlordiazepoxide) • Better for low potency benzodiazepines
Medicating Benzodiazepine Withdrawal Syndrome - 2 • Timeframe: Medium length (3 to 10 weeks) • Process: 1. Stabilize for 2 to 3 days on equivalent dose of phenobarbital 2. Taper over 3 to 10 weeks • Reduce phenobarbital weekly • Initially by 30 to 60 mg/week then 15 mg • Adjust taper speed by patient response
Medicating Benzodiazepine Withdrawal Syndrome - 3 • First day goal: determine phenobarbital equivalence dose • Track progress with same single question • Frequently cannot achieve zero level of comfort • Inform patient that reason is to avoid cross-addiction
Medicating Benzodiazepine Withdrawal Syndrome - 3 • Be alert to danger of plateau instead of taper • Watch for co-occurring anxiety disorder that may require treatment • Consider early use of non-addicting anti-anxiety medication
3. Opioid Withdrawal Syndrome: Time Frame After Last Use • Short acting (heroin, oxycodone, hydrocodone) • Onset: Within 4 to 6 hours of cessation • Peak severity: 36 to 72 hours • Duration: 7 to 14 days • Long acting (methadone) • Onset: Within 36 hours of cessation • Peak severity: 10 to 14 days • Duration: 6 or more months
Medicating OpioidWithdrawal Syndrome - 1 • Time Frames: 1. Taper over 1 to 4 weeks • Better results with one month than with one to two weeks 2. Stabilization: continue for one year 3. Maintenance: continue indefinitely • Tracking Progress • Use same single question
Medicating OpioidWithdrawal Syndrome - 2 • Medication choices • Best: Suboxone (buprenorphine) • Alternative: tramadol (Ultram) • Traditional: methadone or clonidine + sedative
Buprenorphine Features • Partial opioid agonist • Compounded with naloxone to discourage IV use, not for opioid blockade • Advantages over methadone • No overdose due to ceiling effect • Less sedation and euphoria • Legal to prescribe in the office by qualified physician (Must have 8 hours training)
Buprenorphine: Avoiding Extremes • Diversion of the mono-product when injected has been a problem outside of USA • Some evidence that history of street diversion in USA is associated with better treatment outcomes • Analogy: like anesthesia for surgery
Buprenorphine Protocol • 4 mg hourly until symptoms remit • Daily range 8 to 24 mg • Lower dose for induction than detoxification • Begin with 2 mg • Limited use for methadone doses > 30 mg and high oxycodone doses (>400 mg) • Can taper over 1 to 4 weeks but longer term stabilization for months is preferable
Buprenorphine Websites • www.buprenorphine.samhsa.gov • www.naabt.org
4. Tobacco Withdrawal Syndrome Issues • Major barrier to initiating abstinence • Most people do not last 48 hours • Persistent: discomfort lasts for weeks • Paying for medications • Insurance coverage varies • Free: • Best: Baltimore County residents and employees • National quit line: 1.800.QUITNOW (784-8669)
Medicating Tobacco Withdrawal Syndrome: Chantix, Wellbutrin • Chantix (varenicline): nicotine receptor agonist • Relieves withdrawal symptoms • Blocks reinforcing effect of nicotine • Side effects: nausea, vivid dreams, psychological discomfort • Reduce by increasing dose gradually • Wellbutrin/Zyban (buproprion) • Mechanism of action not clear • Not as effective as Chantix • Well tolerated
Medicating Tobacco Withdrawal Syndrome: Nicotine Replacement • Long acting: patch (1mg. per # of cigarettes per day) • Short acting • Non-prescription: gum, lozenges • Prescription: Nicotrol “inhaler,” nasal spray • Electronic cigarette: newer and less studied
Medicating Tobacco Withdrawal Syndrome: 3 Level Approach • One week before quit date: start Chantix 2. Night before quit date: put on patch • In morning, replace patch • New patch each morning • For cravings: use inhaler, gum, or lozenges • Time Frame: “as long as it takes”
Double Withdrawal Strategies:Alcohol and Opioids • Simultaneous is feasible: • Benzodiazepines remove ceiling effect of buprenorphine • Use with caution or consider carbamazepine
Double Withdrawal Strategies:Split • Opioids and benzodiazepines • Stabilizing opioids before withdrawing from benzodiazepines • Alcohol and benzodiazepines • Withdrawal from alcohol and delay benzodiazepines
Antabuse (disulfiram) • Discourages drinking through awareness of unpleasant reaction • Interferes with breakdown of alcohol dehydrogenase and causes transient increase in acetaldehyde • Dose: 125 to 250 mg/day • Not routinely hepatotoxic • Allergic hepatitis uncommon • Detected at 4 weeks: increased ALT > AST
Vivitrol/Revia (naltrexone) • Reduces craving and alcohol euphoric effect • Reduces stimulating effect of alcohol on endogenous opioid, which reduces effect on dopaminergic reward system • For patients with strong family history of alcoholism • Dose: 50 to 100 mg/day • Liver toxicity exaggerated
Naltrexone Induction(Drops: 50 mg/100 ml) • Opioids (can begin day after last opioid use) • Day 1: 5 drops, repeat in one hour • Day 2: 10 drops, repeat in one hour • Day 3: 1/8 tablet (6.2 mg) • Day 4: ¼ tablet (12.5 mg) • Day 5: ½ tablet (25 mg) • Day 6: full tablet (50 mg) • Alcohol (wait 1 to 2 days after last drink) • Day 1: ¼ tablet • Day 2: ½ tablet • Day 3: full tablet
Campral (acamprosate) • Reduces relapse by decreasing thoughts of alcohol and power of triggers • Modified taurine molecule dampens glutamatergic hyperactivity following alcohol withdrawal • Target is abnormal metabolism of alcoholic • Dose: 666 mg 3 times daily • High safety level: not metabolized, excreted by kidney, no reaction if patient drinks
Use Long Acting Benzodiazepines • Librium 50 mg.= Valium 20 mg.= Serax 20 mg. • Do not use I.M. because they are poorly absorbed • Initial relief may require as few as 1 or as many as 5 doses • After the first day, begin to taper and give only once or twice daily, weighted toward bedtime to facilitate sleeping
Symptom Triggered Librium Protocol • First day: Librium 50 mg hourly until anxiety is relieved or mildly sedated (50 to 300 mg) • First night: Librium 50 mg at bedtime • Repeat hourly x 2 until asleep • Second day: Librium 50 mg x 1 – 2 in A.M. • Only if very anxious • Second night: Librium 50 mg at bedtime • Repeat in one hour if not asleep • Third night: Librium 50 mg at bedtime if needed