Download
1 / 27
270 likes | 379 Vues
PRIORITY MEDICINES FOR EUROPE AND THE WORLD . Warren Kaplan Richard Laing Other WHO Participants:. Saloni Tanna Marjolein Willemen Eduardo Sabaté Monique Renevier Joyce Wilson Lisa Greenough Ann Wilberforce Kathy Hurst. Objectives/Deliverables.

E N D
PRIORITY MEDICINES FOR EUROPE AND THE WORLD Warren Kaplan Richard Laing Other WHO Participants: • Saloni Tanna Marjolein Willemen • Eduardo Sabaté Monique Renevier • Joyce Wilson Lisa Greenough • Ann Wilberforce Kathy Hurst
Objectives/Deliverables • Provide a methodology for identifying priority diseases with pharmaceutical “gaps” from a public health perspective, for Europe and the World . • Provide a public-health based pharmaceutical R&D agenda for use by the EU in the 7th Framework Programme, which includes research into barriers to pharmaceutical innovation and ways of overcoming such barriers. • Provide a Report for 18 November “Good public policy aims to prioritise spending of public funds on areas of greatest public needs”
Priority Medicines Project • Background/Introduction • Priority Setting • Methods • Results/Conclusions
"Priority Medicines" • Medicines which are needed to meet the priority health care needs of the population (“essential medicines”) but which have not yet been developed. • For the purposes of this Report, a "priority" medicine for a priority disease is by definition also a significant improvement over already-marketed products
Pharmaceutical "Gaps" pharmaceutical treatments for a disease/condition which: • does not yet exist OR • are likely to become ineffective in the future OR • are available but the delivery mechanism or formulation is not appropriate for the target patient group.
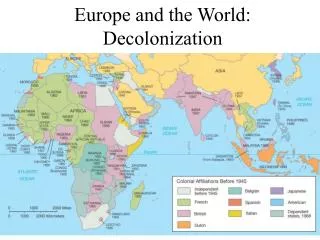
Context/Background • Pammoli, G-10 and EU Commission Reports • Europe was “lagging behind in its ability to generate, organize, and sustain innovation processes that are increasingly expensive and organizationally complex.” • The Lisbon and Barcelona European Councils: the “3% solution” • Responses by EMEA : "Roadmap to 2010…" • US FDA "Innovation or Stagnation…?" • Framework Programmes • European and Developing Countries Clinical Trials Partnership (EDCTP)
100% Untreatable with existing interventions including incurable chronic conditions 4 1 2 3 Combined efficacy of a mix Treatable with current Treatable with Few treatments of all mix of interventions existing interventions available, better available but obstacles to formulations and interventions access exist delivery mechanisms needed 0% Population coverage 0% 100% with current mix Maximum achievable of interventions coverage Identifying gaps (unmet therapeutic needs):a public health perspective
What this Report does not address • Health system issues such as access or quality of care, or logistical or sociological barriers. • Obesity as an underlying risk factor which can be considered a major cause of morbidity or mortality. • Availability of diagnostics or medical devices • Relationship between trade, pricing, intellectual property, as this is the subject of the WHO Commission on Intellectual Property Rights, Innovation and Public Health. (See http://www.who.int/intellectualproperty/en/)
Priority Medicines Project • Background/Introduction • Priority Setting • Methods • Results/Conclusions
International organizations and less formal groups have developed methods for prioritizing health research • The Commission on Health Research for Development (1990) • The World Development Report (1993 ) • The Ad Hoc Committee on Health Research (1996) • The Global Forum for Health Research (2000) • WHO-IFPMA Round Table (2000-2001) • The UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (TDR) • The US National Institutes of Health (NIH) (1998)
Source: Adapted from Dr. Kenneth Hammond, Univ. Colorado, USA Prioritization must be multifactorial
Priority Medicines Project • Background/Introduction • Priority Setting • Methods • Results/Conclusions
In-depth Reviews • What is the size and nature of the disease burden? • What is the control strategy? • Why does the disease burden persist? • What can be learnt from past/current research into pharmaceutical interventions for this condition? • What is the current “pipeline” of products that are to be used for this particular condition? • What are the opportunities for research into new pharmaceutical interventions? • What are the gaps between current research and potential research issues which could make a difference, are affordable and could be carried out in a) five years or b) in the longer term? • For which of these gaps are there opportunities for pharmaceutical research?
Priority Medicines Project • Background/Introduction • Priority Setting • Methods • Results/Conclusions
Results (1) "Commonality of interest"
Results (2) Global Public Health Threats Antibiotic Resistance: • For acute diseases, particularly infectious diseases, the burden in Europe is low. • Healthcare systems are only slowly "rationalizing" antibiotic use • Most antibiotics are inexpensive- less robust market incentives to create new antibiotics • Less research on antibiotics could have profound consequences for future generations in view of the global increase in the spread of drug-resistant bacteria. Pandemic Influenza: • Overdue for a new pandemic • Uptake of existing vaccines is poor • Current capacity to produce either vaccines or antiviral medicines is not sufficient
Results (3) High burden, preventable diseases with pharmaceutical gaps Smoking-related conditions: • Public health, anti-smoking policies are the key interventions • Pharmaceutical interventions to stop smoking may be useful adjuncts and better products are needed. • For COPD, translational research to convert basic science advances into products that can be used in clinical trials. Secondary prevention of cardiovascular disease: • The "polypill" concept using fixed dose combinations deserves further study. Treatment of acute stroke: • A major basic and clinical research effort is required as the current treatment of acute stroke is unsatisfactory. • Most agents are not effective and they are associated with an increased risk of adverse events.
Results (3 continued) High burden, preventable diseases with pharmaceutical gaps HIV/AIDS: • There are particular "gaps" with regard to pediatric HIV formulations Alcoholic liver disease: • The overriding imperative should be to reduce the prevalence and incidence of drinking. • Need for translational research to convert basic science advances on fibrosis into products that can be used in clinical trials.
Results (4) High burden diseases without cure Osteoarthritis: • New diagnostics, biomarkers and imaging technology will help the medical community to determine who is likely to get arthritis, the severity and progression of disease, and the response to medicines. Alzheimer disease: • More sensitive, reliable and valid tools for detecting changes in normal ageing and the onset of early Alzheimer disease. • Lack of surrogate markers as therapeutic endpoints remains a major barrier in the clinical development of efficacious AD drugs
Results (5) High burden diseases where existing therapies could be improved Cancer : • More capacity (infrastructure and human resources) and coordination to conduct comparative Phase II/III clinical trials • Continue to invest in basic research into cancer biology Type 2 Diabetes: • Heat stable insulin would be a major advance in public health • Increased infrastructure to facilitate diabetes clinical trials, in particular comparative clinical “head-to-head” trials Type 1 diabetes: • Gaps in basic biology, stem cell research, transplantation research Depression in children/elderly: • Gaps in understanding biology of depression and its treatments in these groups
Results (6) "Neglected" diseases Malaria: • Lack of cost efficient experimental models for medicines discovery and development. • Weak EU creation and funding of new partnerships toward translational research Tuberculosis: • More FDCs for second-line treatment of multidrug-resistant TB • Weak EU creation and funding of new partnerships toward translational research Leishmaniasis, trypanosomiasis, Buruli ulcer: • Most of the medicines being used are "old" and often dangerous • Weak EU creation and funding of new partnerships toward translational research Post-partum haemorrhage: • A significant cause of maternal mortality in developing countries, heat stable oxytocin would be a major advance in public health
Infections due to antibacterial resistance Pandemic Influenza Smoking-related diseases/interventions for smoking cessation Cardiovascular disease Diabetes Cancer Acute stroke HIV and AIDS Tuberculosis Neglected diseases Malaria Alzheimer disease Osteoarthritis Chronic obstructive pulmonary disease Alcohol dependency, alcohol liver disease Depression in Children and the Elderly Postpartum hemorrhage Conclusions: Preliminary List of Priority Diseases for which "priority medicines" are needed
Priority Medicines Project For further questions, please do not hesitate to contact us at: Laingr@who.int wak22@comcast.net +41-22-791-4533 http://mednet3.who.int/prioritymeds/interimReport_04_2004/index.htm