Download
1 / 57
580 likes | 766 Vues
The Future of Sleep Apnea Therapy Atul Malhotra, MD (amalhotra1@partners.org) Associate Professor of Medicine Medical Director, Sleep Program Clinical Chief, Sleep Division BWH and SHC Harvard Medical School NESS 2010. Inadequate Anatomy Compensatory Reflex Activity of

E N D
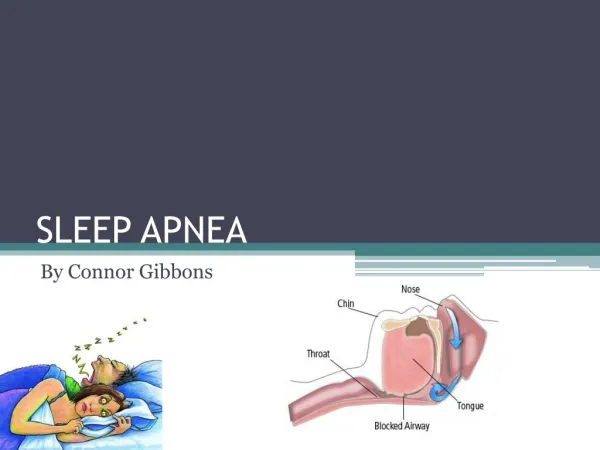
The Future of Sleep Apnea Therapy Atul Malhotra, MD (amalhotra1@partners.org) Associate Professor of Medicine Medical Director, Sleep Program Clinical Chief, Sleep Division BWH and SHC Harvard Medical School NESS 2010
Inadequate Anatomy Compensatory Reflex Activity of Pharyngeal Dilators (GG) Sleep Fragmentation Neurocognitive Sequelae Airway Collapse Endothelin Vagus Cardiovascular Sequelae Maintains Upper Airway Patency Sympathetic Activation Sleep Onset Arousal Loss of Reflex Respiratory Effort Activity of Pharyngeal Dilators Hypoxia + Hypercapnia Malhotra and White Lancet 2002
Current Standard Therapy is CPAP • Treatment of choice meta-analysis, SLEEP 2003 • Improves symptoms and blood pressure • Adherence is variable
Alternative Therapies • Bi-level – no convincing data • APAP – Patel et al. SLEEP 2004 • Cflex – Aloia et al. Chest 2005 • CRT in CHF – Stanchina et al. Chest 2007 • Oral appliances – variable response, limited data • Surgery – poor efficacy, minimal ability to predict who will respond
OSA Pathogenesis Patients do not all get OSA for the same reason. There are likely to be multiple mechanistic pathways and we need to recognize and target them. Owens et al. SLEEP 2009; Saboisky Thorax 2010
Obstructive Sleep Apnea Underlying Mechanisms • Anatomy • Pharyngeal dilator muscle control asleep • Arousal Threshold • Loop gain • Lung volume • Vascular
Pharyngeal anatomy explains only a minimal portion of the variability in AHI
Finite Element Modeling • 1. Upper airway mechanics: influence of gender IEEE 2002 • 2. A pressure and state-dependent muscle contraction model and its application in the computational simulation of human upper airway collapse JAP 2005 • 3. Mandibular advancement and UPPP effects on pharyngeal mechanics based on FEA IEEE 2003 • 4. The impact of anatomical manipulation on pharyngeal mechanics: results from a computational model, Chest 2005 • 5. Invididualizing Therapy Laryngoscope 2007
Finite Element Modeling • Signal average MRI • Muscle contracts per experimental data • Tissue elastic modulus derived from back calculations from the literature • Allows tissue displacement and air-solid interactions • Measure Pcrit as primary outcome variable
Mandibular Advancement A 1-cm mandibular advancement has a substantial impact on collapsibility:P close = -21 cmH2O with; -13 cmH2O without mandibular advancement Huang, White and Malhotra, Chest 2005
Huang, White and Malhotra Chest 2005 Uvula Removal Uvula removal can have a substantial effect on collapsibility:P close = -18 cmH2O with uvula removal; -13 cmH2O with intact uvula.
Airway Length • Normal men have longer airway than women (Malhotra et al. AJRCCM 2002) • Boys develop longer airway at puberty as compared with girls (Ronen et al., Pediatrics 2007) • Women experience airway lengthening at menopause (Malhotra et al. AJM 2006) • OSA patients also have gender differences in some data sets (Pillar et al., S & B 2008) • Modeling shows that length affects mechanics • Airway length may explain considerable variance in airway mechanics and components of various epidemiological risk factors
Science Fiction? • Can we individualize therapy based on imaging? • Our imaging collaborators do intraoperative MRI during craniotomy to simulate brain deformation following tumor resection • Neurosurgeons are now using this in real time to determine the extent of tumor resection • Requirement that individual anatomy can be down-loaded into the FEA model
Obstructive Sleep Apnea Underlying Mechanisms • Anatomy • Pharyngeal dilator muscle control asleep • Arousal Threshold • Loop gain • Lung volume • Vascular
Pharyngeal Motor Control Studies • 1. Genioglossal But Not Palatal Muscle Activity Relates Closely to Pharyngeal Pressure Malhotra et al. AJRCCM 2000a,2000b AJRCCM 2002 • 2. Within-breath control of genioglossal muscle activation in humans: effect of sleep-wake state J. Physiol. 2003 • 3. Control of upper airway muscle activity in younger vs older men during sleep onset J. Physiol. 2004 • 4. The impact of wakefulness stimulus on pharyngeal motor control Lo et al Thorax 2007 • 5. Mechanisms of Compensation Jordan et al Thorax 2007, Sleep 2009
Malhotra et al. AJM 2006 R=-0.55, p<0.001
Single Motor Units and SFEMG • Wilkinson et al. SLEEP 2008 • Saboisky et al. J Physiol. 2007 • Saboisky et al. J Neurophysiol. 2006 • Wilkinson et al. SLEEP 2010 • High frequency sampling of EMGs • Can “see” activity of single cells in humans • Has opened possibility of pharmacological targets
Pharyngeal Muscle Control • There are likely to be subgroups of patients who respond to efforts to augment muscle activation • Perhaps targeting this subgroup would make sense in pharmacological studies (JAP 2008) • Increasing upper airway muscle responsiveness may be deleterious in patients with unstable ventilatory control
Obstructive Sleep Apnea Underlying Mechanisms • Anatomy • Pharyngeal dilator muscle control asleep • Arousal Threshold • Loop gain • Lung volume
Arousal Threshold – Double-edged Sword • A low arousal threshold could lead to premature arousal with inadequate time to accumulate respiratory stimuli (CO2 and neg pressure) • A high arousal threshold could lead to substantial hypoxemia and hypercapnia with end-organ impact • Therapies to manipulate arousal threshold are likely to benefit some patients and theoretically hurt others Saboisky et al. Thorax 2010
Arousal Threshold • Agents that increase arousal threshold e.g. sedatives can prevent state instability Younes et al SLEEP 2007 Park et al SLEEP 2008 • Certain patients who arouse easily may be more amenable to these than others • Ideally the agent does not suppress UA muscle activity • Delaying arousal may allow time for UA muscles to ↑ • Most OSA patients have some periods of stable breathing • UA muscles are necessary and sufficient to stabilize breathing (SLEEP 2009)
Most OSA patients have spontaneous periods of breathing stability • Studied GGEMG, TPEMG, EELV etc Sleep 2009
Pharmacology Studies of Sedation/Anesthesia in Rats • Unwarranted Administration of Acetylcholinesterase Inhibitors Can Impair Genioglossus and Diaphragm Muscle Function. Anesthesiology 2007 • Differential effects of isoflurane and propofol on genioglossus muscle function and breathing. Anesthesiology 2008 • Sugammadex Brit J. Anesth. 2008 • Pentobarbital Anesthesiology 2009 • Rocuronium vs. Cisatracurium AJCC 2009 • Pentobarbital in humans ERJ in press • Agents have differential effects on the upper airway Chamberlin et al.
Obstructive Sleep Apnea Underlying Mechanisms • Anatomy • Pharyngeal dilator muscle control asleep • Arousal Threshold • Loop gain • Lung Volume • Vascular function
Loop Gain • measure of the stability of negative feedback control system Younes AJRCCM 2001 Wellman et al JAP 2003 Wellman et al AJRCCM 2004 Wellman et al J Physiol 2007 Wellman et al. Resp Physiol 2008 Jordan et al J Physiol 2004 Jordan et al JAP 2006
r = 0.36 p = 0.076
r = 0.88 p = 0.0016 AJRCCM 2004
Change in Ventilatory Effort Across an Obstructive Apnea PN E2 E1 ABD Effort Index = (E2 – E1) / E2
Effort Index may be a Reasonable Surrogate for Loop Gain 1 R = 0.96 0.8 P < 0.05 Effort Index 0.6 0.4 0.2 0 0 0.2 0.4 0.6 0.8 1 1.2 Loop Gain
Obstructive Sleep ApneaFuture Treatment • Define the apnea mechanism and treat accordingly.