Download
1 / 41
410 likes | 572 Vues
NCDR Update Board of Governors Meeting September 16, 2007. John Brush, MD, FACC Chair, Quality Strategic Directions Committee ACC Governor, Virginia Chapter. 20 Years of Performance Measurement. 1987. 1997. 2007. Hospitals Physicians. HCFA CCP Pilot. JCAHO ORYX. IOM Rpt. CED.

E N D
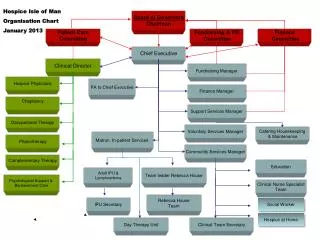
NCDR Update Board of Governors Meeting September 16, 2007 John Brush, MD, FACC Chair, Quality Strategic Directions Committee ACC Governor, Virginia Chapter
20 Years of Performance Measurement 1987 1997 2007 Hospitals Physicians HCFA CCP Pilot JCAHO ORYX IOM Rpt CED IOM Rpt HCFA hospital mortality reports AQA Healthgrades Leapfrog JCAHO “Agenda for Change” QPM to CMS HCFA HCQII HCFA National CCP NQF IOM Rpt QPM to JCAHO JCAHO Core Pilot PQRI HCFA 6 Nat’l Conditions NCQA HEDIS measures NCQA website JCAHO Core Measures
QCAREACC’s Commitment To You • Continuous review of new science • Evidence-based guidelines and standards • Comprehensive education • Data reporting and collection through registries (NCDR) • National Quality Initiatives (D2B) • Adoption and appropriate use of new technology • Evaluation through self-assessment tools, performance testing and longitudinal studies
QCARE Q
Ped. Registry Imaging CHD EP Registry ICD Long PracMgt Registry IC3 CAD Office ACTION Registry PAD Registry CARE Registry ICD Registry HF Registry CathPCI Registry 1997….. 2004 2005 2006 2007 2008 beyond
Partners CathPCI • Society for Cardiovascular Angiography and Intervention ICD • Heart Rhythm Society CARE • Society for Cardiovascular Angiography and Intervention • Society for Interventional Radiology • American Academy of Neurology • American Academy of Neurosurgery • Society of Vascular Medicine and Biology ACTION • In discussion with American Heart Association
Registry/QI • >950 hospitals • 6 million patient records • Online data entry tool launch 4/07 • Support D2B Alliance ARS • States – MA, OH, WV, ?CT, ?NJ • Payers – United, BCBSA, WellPoint Research and Publications • DCRI analytic center • 8* abstracts at AHA
Registry • 1450 enrolled • 150,000 patient records Funding • 2007 support from WellPoint • $1,895/year ARS • UHC added ICD Registry participation for sites with EP Labs • Discussions underway with BCBSA • Provide data to CMS for reimbursement Research • ICD Longitudinal Study • Performing analysis for FDA
Registry • 235 Participants • Data entry tool • $3195.00/year ARS • CMS required Research • Performing analysis for FDA • Discussion with CAS makers re: PMS
Registry • 250+ participants • No charge • Funding provided by • Genentech • Bristol-Myers Squibb/Sanofi Partnership • Schering Plough Corporation ARS • Early discussions with payers
ACTION Registry™ (Acute Coronary Treatment and Intervention Outcomes Network)Initial Report1st Quarter 2007 Results
2006-07 Data Submission Summary Admission # of # of # of Timeframe Sites NSTEMI Records STEMI Records ACTION Jan. 1, 2007 – 227 6,917 4,259 Mar. 31, 2007 CRUSADE April 1, 2006 – 280 20,084 4,391 Dec. 31, 2006
ACTION Registry 2007 Patient Enrollment Number of Patients enrolled
NSTEMI Patient - Baseline Characteristics NSTEMIVariable(n = 26,902) Mean age ± SD (yrs) 69 ± 14 Female 40% Diabetes mellitus 33% Prior MI 29% Prior CHF 16% Prior PCI 23% Prior CABG 19% ACTION/CRUSADE DATA: April 1, 2006 – May 31, 2007 (n=26,902)
In-Hospital Outcomes VariableNSTEMI (n = 26,902) Death 3.8% Re-infarction 1.5% CHF 6.8% Cardiogenic Shock 2.4% Stroke 0.7% RBC Transfusion* 8.9% *Excluding CABG patients ACTION/CRUSADE DATA: April 1, 2006 – May 31, 2007 (n=26,902)
NSTEMI Acute Medications ACTION/CRUSADE DATA: April 1, 2006 – May 31, 2007
NSTEMI Discharge Medications % Use *LVEF < 40%, CHF, DM, HTN# Known hyperlipidemia, TC, LDL ACTION/CRUSADE DATA: April 1, 2006 – May 31, 2007 (n= 26,902)
CathLab Congenital Heart Disease Registry • Transcatheter device occlusion of CV malformations • Atrial Septal Defect • Ventricular Septal Defect • Patent Ductus Arteriosus • Fistula/Collateral Vessels—Blood Vessel Communication • Closure of Fontan Fenestration • Transcatheter Balloon Dilation • Transcatheter Stent Placement
Pilot StudyEvaluation of Appropriateness ofSPECT MPI The American College of Cardiology The American Society of Nuclear Cardiology
SPECT MPI Registry Objectives • Evaluate appropriateness • Promote awareness of appropriateness criteria in practice • Provide feedback reports to improve both practice-level and individual physician-level adherence to the criteria • Establish benchmarks to guide performance improvement
NCDR QI NCDR & D2B Take ACTION Field Consultants • National QI Programs • Implement guidelines recommendations • Improve physician adherence • Improve patient compliance • Our Goal? • Reduce complications • Improve Structure and Process • Efficient Systems
“Take ACTION” Campaign • Nationwide QI Program • Increase awareness about relevant CPG recommended therapies for ACS and chronic stable coronary disease • Improve physician adherence and patient compliance • Long-term Goal • Reduce secondary events post ACS • Measured incrementally through behavioral changes • Multiple, overlapping Phases beginning ACC.07 • Phase I - What is the ACC doing to Take ACTION to improve care of patients with ACS? • Phase II - What are you doing as a physician to Take ACTION? • Phase III - What are you doing as patients to Take ACTION?
ACC-NCDR IC3 ACTION IC3 ACTION Follow-up Measuring the Continuum of CAD Care AMI Care Post-Hospitalization: Risk factor modification Cardiac rehabilitation Patient with stable angina Onset of Acute Coronary Syndrome D/C Admit PCI/CABG
The IC3 Program • First office-based registry designed to assess physician adherence to ACC/AHA Performance Measures. • Provides a powerful tool to assess the current state of office-based clinical care for CAD and CHF patients.
Philosophy of the IC3 Program • Make it easier for busy clinicians to do the right thing for the right patient at the right time • Track key performance measures for CAD/CHF • Internal QI and P4P reporting at the practice level • Performance measures for DM also captured • Make care more efficient • A worksheet that readily identifies opportunities to apply CAD/ CHF guideline recommendations and performance measures • Coordinate care • Create a visit summary to communicate with patients and other providers
IC3 Program: Incentives for Practices • Develop tools to improve care • Provide real-time reporting of office-based quality indicators for CAD and CHF derived from clinical practice guidelines • Create a trusted mechanism for measuring performance • Support evolving CMS outpatient quality measures and regulatory reporting initiatives • Support Pay-for-Performance programs with payers
Physician X’s Practice Payer Perspective of my Performance United (5) 40% BCBS (9) 76% Medicare (26) 100% Medicaid (10) 100% Physician X’s Overall Performance = 90%
Partnering with Health Plans – Benefits to Plans… • Health Plans get Better Picture of Practice Performance • Clinical data prospectively measured • More accurate assessment of practice performance from larger sample sizes than individual plans • Capture of complete ACC/AHA performance measures • Plans need not develop their own
Other IC3 Program Goals • Position the profession (ACC) to take a leadership role in quality assessment and improvement • Support the evolution of quality assessment and improvement • Identify new opportunities to improve and coordinate CAD and CHF care • Create a research agenda to improve care • Document the distribution of cardiac patients’ health status • Identify new performance measures • Support research of appropriateness
Data Entered through NCDR IC3 Office Flow in IC3 Data entered and Clinic Visit Form Generated Treatment plan Data entered Pt presents for visit, reports med changes Vitals, health status assessed Physician Visit & Rx Patient Letter & Visit Summary dispensed Visit Summary sent to other care providers
Data Collection • Types of data • Site Profile captured once • Patient History captured on entry • Treatment monitored longitudinally • Clinical event data captured longitudinally • Patient health status for CAD and CHF (optional) • Data collection tools • Web-based data collection tool • Paper forms • Working on EMR integration for Decision Support
Data Submission and Reporting • Data will be subjected to completeness and consistency reviews • On-site audit to ensure accuracy (2009) • Quarterly aggregate practice-level data reports and benchmark reports • National benchmark performance • Peer group benchmark performance • Individual hospital performance • Real-time QI reports generated for individual and practice-level data
Release • Enrollment begins October 1, 2007 • Web-based data collection begins Jan 1, 2008 • Training and roll-out for participants • Client and contract support for participants • Marketing and communications to broader physician community
Participant Training and Education • NCDR Online website • Information packet/Welcome Kit • Online training manual • Annual User Group Meeting • Workshops • Special web casts • On-line community development for collaborative learning and sharing
For More Information… Visit: www.ncdr.com/ic3 Email: ncdr@acc.org