Download
1 / 18
180 likes | 252 Vues
Learn about the various treatment options for low grade lymphomas, including watchful waiting, radiotherapy, chemotherapy, monoclonal antibodies, radioimmunotherapy, and stem cell transplantation. Explore new agents like Ibrutinib, Idelalisib, Venetoclax, and Obinutuzumab. Understand the mechanisms of action and targeted therapies involved in managing follicular lymphoma.

E N D
Low Grade Lymphomas:Treatment approaches Parameswaran Venugopal, MD Professor of Medicine Rush University Medical Center
Relative Incidence of NHL Subtypes Armitage and Weisenburger. J Clin Oncol. 1998;16:2780. Adapted from Jemal et al. CA Cancer J Clin. 2006;56:106.
Selected Indolent B-Cell Non-Hodgkin’s Lymphoma Subtypes *%of all NHL. National Comprehensive Cancer Network. Practice Guidelines in Oncology. v.2.2006. At: http://www.cancer.gov/cancertopics/pdq/treatment/adult-non-hodgkins/HealthProfessional/page2. Accessed May 2006. Ansell and Armitage. Mayo Clin Proc. 2005;80:1087.
Indolent lymphoma accounts for 30%-40% of NHL cases FL (22%), SLL (7%), MALT (8%), WM (uncommon) Often asymptomatic 85%-90% present in stage III or IV (Ann Arbor Staging) Long median survival (~10 years) Advanced disease rarely curable with conventional treatments Transformation to aggressive lymphoma often occurs 3% risk/year 30% risk over 10 years Low Grade Lymphoma Winter et al. Hematology. 2004;203. Armitage and Weisenburger. J Clin Oncol. 1998;16:2780. Adapted from Jemal et al. CA Cancer J Clin. 2005;55:10. Al-Tourah et al. ASCO, 2006. Abstract 7510.
Follicular Lymphoma (FL) • Most common indolent NHL, accounts for ~22% of NHL in North America • Typically advanced stage at presentation • Often asymptomatic
FL: WHO/REAL Grading Grade 1 <5/hpf Grade 2 Grade 3a 6-15/hpf Grade 3b >15/hpf Sheet
Follicular Lymphoma: Diagnosis • B symptoms • Physical Examination • Laboratory studies: • Biopsy of Lymph Node • Bone Marrow Biopsy • CAT Scan • PET scan
Watch & WaitRadiotherapyChemotherapyMonoclonal AntibodiesRadioimmunotherapyStem Cell TransplantationNew Agents:
New Agents: Ibrutinib (Imbruvica) Idelalisib (Zydelig) Venetoclax (Venclexta) Obinutuzumab (Gazyva)
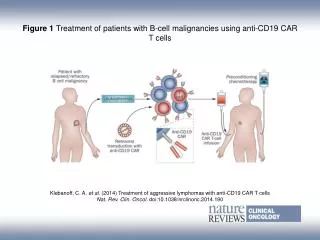
Murine/human IgG1 kappa monoclonal antibody Binds to CD20 antigen Half-life (at 375 mg/m2) ~76.3 hours after 1st infusion and 205.8 hours after the 4th infusion Mechanism of action CDC, ADCC, apoptosis, and ionizing radiation–induced cell death Rituximab as a Targeted Therapy in FL Murine variable regions bind specifically to CD20 on B cells Human constant regions Human IgG1 Fc domain works in synergy with human effector mechanisms CDC = complement-mediated cell death; ADCC = antibody-dependent cell cytotoxicity.
Granules Fc receptor (FcgRIII) Antigen Fc region Antibody NK cell B cell Granules release perforins and granzymes; cytokines secreted (eg, IFNg) Lysis H2O, ions, granzymes Pores (perforin) Antibody-Dependent Cell-Mediated Cytotoxicity (ADCC) NK = natural killer.
Radioimmunotherapy Ibritumomab Tositumomab Chelator Radionuclide Tiuxetan
Targeting of B Cell Receptor Niedermeier M, et al. Blood. 2009;113(22):5549-5557.