Download
1 / 21
210 likes | 242 Vues
Learn about a successful model of HIV intervention among drug users in resource-poor setting of Bangladesh. Explore the strategies, findings, and achievements of the program implemented by UNICEF and CARE Bangladesh.

E N D
IDU interventions in Bangladesh:An example of a successful model from a resource-poor setting Dr. Munir Ahmed MBBS, MPH, Dip in HE Team Leader-UNICEF-HAPP HIV Program, CARE Bangladesh
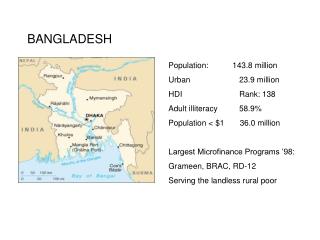
Bangladesh Country profile • Area: 148,000 Sq. Km (Census-2001) • Pop: 130 million(Census-2001), Growth rate = 1.48 • 88% Muslim • GDP:US$ 55.4 Billion (BBS,Bd. Bank, Finance ministry) • Per Capita Income: US$444 • EconomicGrowth rate: 5.52% (BBS,BB, Finance Ministry) • Agro-based country • RMG, jute and jute products, manpower export are major wage earners. • Source:Bangladesh Demographic and Health Survey(BDHS)
Bangladesh Health Indicators • MMR: 3.2/1000(2001) • IMR: 65(2004) • TFR: 3 (2004) • CPR:58.1% (2004) • Annual Health Budget per person: US$1.61 • Source:Bangladesh Demographic and Health Survey(BDHS) • Life Expectancy: Male=68, female=68.6 • Source: BBS-2001
GoB Policy on drug use • Existing Law: • Carrying of Heroin less than 25 gm is punishable with 2-10 yrs imprisonment. • More than 25 gm - death penalty or life imprisonment • Carrying of pathedine, morphine, methadone, cannabis all are punishable crime. • Possession of injecting paraphernalia is also a punishable crime. • Source: Narcotics Control law,1990, GoB. NSEP not legal as per narcotics law
National Strategic Plan for HIV/AIDS 2004-2010 • Five Objectives: • Provide support and services to the priority groups of people. • Prevent vulnerability to HIV infection in Bangladesh society • Promote safe practices in the health care system. • Provide care and support services for PHAs. • Minimize the impact of the HIV/AIDS epidemic.
Cont’d… Sub component of Objective one is to provide support and services to drug users • 5 strategies: • Strengthen research on drug use • Strengthen harm reduction programs • Learn how drug use influences sexual behaviour. • Slow entry into drug use • Political, bureaucratic and legal support for effective programming
Background of CARE Bangladesh IDU program • HIV/AIDS included as programming initiative for Health and Population Sector of CARE-B in its multi-year planning document for 1993-2000 • 1993-94: HIV/AIDS orientation for 1600 staff • July 16, 1995: SHAKTI project launched (IDU component from 1998)
Baseline Study-1998 • Objectives: • Determine nature and magnitude of drug injecting in Dhaka • Study HIV risk behaviors of IDUs • Study harmful health consequences of drug injecting or other HIV risk behaviors • Determine interventions needed for HIV prevention among IDUs and their sex partners • Identify factors that may facilitate or constrain interventions
Major findings • Estimated number of IDUs: 5000 • Drug of choice : Injection (Buprenorphine) • Sharing of Syringe/Needle: >90% • Homeless IDUs: 30% • No education: 46% • Income: Tk 3000/month ($50USD) • Ever arrested by police: 84% • Ever been to jail: 66% • Ever been assaulted in the street by Police/Public: 57% • Syphilis: 12.9%
HIV Prevalence of IDUs in 5th Rounds of National Sero-surveillance
Evolution of Bangladesh IDU program 1997: Explored preliminary information related to drug injecting in Bangladesh 1998: 1st ever RSA done in Dhaka. Started harm reduction intervention 2000: SHG-concept for current IDUs conceived/ materialized Community based detox arranged with fullest cooperation of DNC/CTC. 2002: Inclusion of HSs, COHORT Started 2003: Intervention for ILWHAs 2004: DRE started, focus on female & child DUs.
2004 2004 2004 2004 2004 2004 2004 2001 1999 2004 2004 2001 2003 2004 2004 1998 2002 2004 2003 2004v 2004 2004 2004 Year wise expansion
CARE-B DUI at a glance (2005): Total fund available: US$1.5 Million in last FY Districts covered =23 DIC = 59 Under coverage: IDU = 6000 plus HS = 10000 plus • 47 staff • 355 OWs • 40 Counselors • OW:IDU - 1:50 • OW:HS - 1:80
Team Leader Technical Coordinator PM/PDO/ PO Field Trainer DIC in Charge Field Supervisor Medical Assistant Dresser Guard Outreach Worker Organogram
Core Activities 1. Drop in Centers • health services (incl. abscess and STI management) • peer and group education • referral to detox programs • client & family counseling • recreational space • toilet and bath facilities 2. Detoxification • symptomatic management (no drug substitution)
Cont’d… 3. Outreach Activities • NSE • condom distribution • one on one counseling • IEC 4. Creating Enabling Environment: • capacity Building of IDUs self-help groups on technical & negotiating skills • advocacy & lobbing
Laurels achieved by this intervention • Best Performance Award from honorable PM for organizing community-based detoxification camp
Our best practices adopted by others • Outreach Model of Dhaka has been selected/mentioned as a best practice in ‘Preventing HIV/AIDS among drug users Case studies from Asia’ published by UNODC • Many examples and experiences have been incorporated into the WHO guideline for HIV prevention among IDUs • UNODC selected this intervention as a resource/model project for NEP outreach to develop standardized NSEP protocol for South Asian countries.
Source: Presentation of Anna Foss, 14th International HR conference
Why it is a successful model • Cost effective • NEP outreach adopted as a best practice for South East Asia recommended by UNODC • Replicated by other organization • NEP launched despite having no relevant law. • Other restrictive factors like conservative Muslim society and frequent eviction/harassment by law enforces.
Future Plans • Country wide program expansion • Start continuum of care for DUs • Crisis care home for street-based marginalized DUs • Mobile clinic and harm reduction service for DUs • 40 more RSAs • Start service for middle-class DUs • Work more closely with GoB and DNC • Vocational training and social re-integration • Pilot oral substitution of drug for ILWHAs. • Pilot ARV for ILWHAs • To install VCTC centers in hot spots.