Download

1 / 31
310 likes | 416 Vues
This report, authored by Dr. Daniel Weber, MD, examines the significant association between oral health, specifically periodontal disease, and preterm delivery rates. With over 131 million births annually worldwide, and a notable decline in preterm births in the USA, it highlights findings from various studies indicating that oral infections may contribute to increased risks of preterm labor. The implications of maternal oral health on fetal outcomes underscore the necessity for pregnant women to maintain good oral hygiene. The report emphasizes the ongoing research and calls for further investigation into preventive treatments.

E N D
Oral Health and Preterm Delivery Daniel Weber, MD OBGYN In-house Medical Expert Dept of State Commonwealth of Pennsylvania
131,000,000 world births/year 2011 estimate
3,953,590 Births/Year 2011 data
142,000 Births/Year 2011 data
45,300 Pa. Medicaid Births, 2011
USA Preterm Birth Data(<37wk) • 11.73% in 2011 (preliminary data) • 5th consecutive year of decrease • Down 2% from 2010 • Down 8% from 2006 peak
BREAKDOWN OF PREMATURE BIRTHS 1990 34-36 wk 7.3% 32-33 1.4% <32 1.9% CDC/NCHS data, 2005 2005 9.1% 1.6% 2.0%
460,000 Premies/year 80,000 very preterm birth/year in USA (<32 weeks)
“Microorganisms or their waste products obtain entrance of parts of the body adjacent to or remote from the mouth.” -- Focal Infection Theory, Dr Miller, 1891 “Gingivitis exacerbated by the hormonal changes of pregnancy (Pregnancy Gingivitis) is considered the most common oral manifestation of pregnancy and has been reported in up to 100% of pregnant women.” -Dental Manifestations of Pregnancy, Pirie et al. 2007 “When questioned, 36.4% of women in the study felt that the condition of their teeth had deteriorated during pregnancy.” -Dental Manifestations of Pregnancy, Y. Turok, 2007
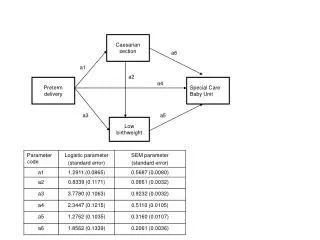
Pregnancy Gingivitis Periodontal Tissues Pathogenic flora leads to endotoxin release, including LipoPolySaccharides Systemic Organs Exposure to LPS and host mediators leading to increased cytokines Periodontal Tissues Local release of inflammatory mediators, IL- lB, TNF-a, PGE2 Fetoplacental Unit Increased IL-IB, PGE2 levels Uterine Contraction Cervical Dilation
mothers withperiodontal infection: • Case control study, 93 mothers • 7 fold increase of PLBW infant (Preterm delivery of LBW infant) • 18% of PLBW infants might be attributable to periodontal disease Offenbacher, J. Periodontology, 1996
Fetal cord blood IgM study • PLBW: 33.3% • Term: 17.9% “Elevated human IgM suggests in utero exposure to periodontal pathogens” Offenbacher, J Dent Res,1999
Oral Conditions And Pregnancy(OCAP) • Clinical data from first 812 deliveries • DNA probes to identify periodontal organisms within maternal periodontal plaque at delivery • Maternal postpartum IgG antibody, and umbilical IgM level to 15 pathogens • Pathogens divided into Orange and Red complexes
OCAP findings • 2.9 fold higher prevalence of IgM for one or more of Orange or Red complexes amongst PTD vs term • + IgM to Campylobacter rectus: 20% for premies, 6% for term. • Lack of maternal IgG antibody to Red complex associated with 2.2 odds ratio of premie. (maternal antibody protecting fetus theory) • 66.7% premature rate with neg maternal IgG to Red Complex, and positive fetal IgM to Orange complex. Madianos, Offenbacher, UNC, Ann Periodontol, 2001
Periodontal Infection and Preterm Birth – Results of a Prospective Study • N = 1313 pregnant patients • Patients with severe or generalized periodontal dz, 4.45 odds ratio for preterm delivery < 37wks • < 35 weeks, odds ratio 5.28 • < 32 weeks, odds ratio 7.07 Jeffcoat, J Am Dent Assoc, 2001
59 pts with preterm birth <32 weeks • 32 pts with indicated preterm birth < 32 weeks • 44 pts with uncomplicated term delivery (>37 weeks) • Association between severe periodontal dz and preterm birth (odds ratio 3.4) • Periodontal dz not associated with selected markers of upper genital tract inflammation (cultures of placenta, umbilical cord blood, cord interleukin-6 levels, and histopathologic placental pathology) Goepfert, Jeffcoat, et.al., Periodontal Disease and Upper Genital Tract Inflammation in Early Spontaneous Birth, Obstetrics & Gynecology 2004
1020 prenatal patients • Preterm birth: 11.2% among periodontally healthy women / 28.6% with moderate-severe periodontal disease • Very preterm birth, <32 weeks: 6.4% with periodontal disease progression vs. 1.8% without disease progression Offenbacher, Obstetrics and Gynecology, 2006
Treatment of Periodontal Disease and the Risk of Preterm Birth • 813 prenatal patients • Treatment group: scaling and root planing, monthly tooth polishing, oral hygiene instruction. • Control group: monthly brief dental exam, treatment pp. • Conclusions: Treatment of periodontitis in pregnancy improves periodontal disease, and is safe, but does not significantly alter rates of PTD, LBW, or IUGR • Delivery <32 wks: control 4.4%, treatment 2.5% • Delivery ,37wks: control 12.8%, treatment 12.0% Michalowicz, DDS, et al, NEJM, Nov 2006
Maternal Oral Therapy to Reduce Obstetric Risk(MOTOR) • NIH funded, 1806 women, 3 sites, opened 2004 • Scaling and root planing in 2nd trimester vs within 4 weeks postpartum. • Offenbacher, UNC • Effect of Periodontal Therapy on Rate of Premature Delivery: A Randomized Controlled Study, (OBGYN Sept 2009) • Conclusion: Perio therapy did not reduce incidence of prematurity
Obstetric outcomes after treatment of periodontal diseaseduring pregnancy: systematic review and meta-analysis Nikolaos P Polyzos; Ilias P Polyzos; Apostolos Zavos; Antonis Valachis; Davide Mauri; Evangelos G Papanikolaou; Spyridon Tzioras; Daniel Weber; Ioannis E Messinis. British Medical Journal December, 2010
Polyzos meta-analysis conclusions Treatment of periodontal disease with scaling and root planing cannot be considered to be an efficient way of reducing the incidence of preterm birth. Women may be advised to have periodical dental examinations during pregnancy to test their dental status and may have treatment for periodontal disease. However, they should be told that such treatment during pregnancy is unlikely to reduce the risk of preterm birth or low birthweight infants.
Self Reported Dental Habits and Preterm Birth 1000 consecutive women surveyed during immediate postpartum stay, 2011, Women & Babies, LG Health • demographics • prior OB history • dental home • last dental visit • oral piercing • flossing • brushing • smoking • birth outcome
Dental Habits study, preliminary findings • demographics: 69% white, 18% latino, 6% black. • MA: 51.4% • smokers: 11.7% • Brush once/day 23.6% • Floss: 62% at least 1/week • dental home: 62% • dental visit in this pregnancy: 54% (MA 50%, commercial health insurance 57%) • overall PTB: 8.2%
Dental Habits study, Preliminary Findings • no impact upon prematurity: dental home, dental visit in pregnancy, flossing frequency, oral piercing. • smoking: RR of PTB 2.5, but freq of brushing no additive impact for smokers • brushing 1/day: RR of PTB 2.3
Follow up research opportunities intervention trial: once/day brushers randomized to routine brushing habits vs. BID brushing
Future research opportunities • Micro RNAs: short non-coding molecules expressed in different tissues which regulate transcription of different genes • Highly specific • Very sturdy
Dr. Dan Weber, contact information: weberobgyn@gmail.com