
Frostbite: Definition, Pathophysiology, and Treatment Guidelines
E N D
Presentation Transcript
Definition & Pathophysiology • Localized, cold-induced injury due to freezing of tissue. • Frost nip: localized numbness or parasthesias which resolve with warming, and without residual damage • Two primary mechanisms • Direct cell death from freezing, formation of ice crystals, fluid / electrolyte shifts • Reperfusion injury • Once the tissue is warmed, return of blood flow triggers formation of reactive oxygen species and release of inflammatory cytokines
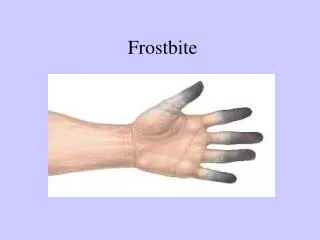
Classification • Grade I • Superficial; focal pallor, numbness, mild swelling • Grade II • Clear-fluid containing blisters, erythema, more swelling, but no tissue loss. • Grade III • Deeper injury, swollen, with hemorrhagic blisters. Can lead to tissue loss. • Grade IV • Complete tissue necrosis, involving muscle and bone, leading to mummification or auto-amputation.
From: Pandey P, Vadlamudi R, Pradhan R, Pandey KR, Kumar A, Hackett P. Case Report: Severe Frostbite in Extreme Altitude Climbers-The Kathmandu Iloprost Experience. Wilderness Environ Med. 2018;29(3):366-374.
Risk Factors • Anything that increases conductive or convective heat loss • Wind, contact with water / metal / ground • Smoking • Previous cold injury • Diabetes, peripheral neuropathy • Intoxication • Maybe females < 20 yrs
Clinical Manifestations • Numbness, clumsiness of the affected extremity. • Before warming, skin may appear gray, dull yellow, and may feel hard or waxy • Any patient with cyanosis proximal to the distal phalanx of any digit after rapid rewarming is at risk for necrosis of the affected tissue and aggressive therapy (eg, thrombolysis in suitable candidates) may be needed.
Treatment (Prehospital) • Transfer patient to warm environment as soon as possible • Avoid walking on frostbitten feet • Remove wet clothing • Avoid rewarming if possibility exists of refreezing • Warm with body heat, clothing, or warm water • DON’T rewarm by rubbing or with heating elements, like a fire or stove
Treatment (Hospital) • Rewarming: ideally using warm water, 37-39C. • Water warmer than 39C / 102F doesn’t result in faster warming, and can worsen tissue damage • Rewarming is complete when tissue is red or purple, generally 15-30 min • Thrombolysis: Inflammation causes clot formation, which worsens perfusion • Severe frostbite presenting within 12-24 hours are eligible for thrombolysis • Patients expected to require significant amputations due to tissue necrosis and who have undergone rewarming within 12 hours injury, without freeze-thaw cycles are eligible for thrombolysis in the absence of contraindications.
Does this actually work? • A single-center, retrospective review of 32 patients with severe frostbite reported that among the six patients (59 digits at risk for amputation) treated with intra-arterial tPA plus intra-arterial heparin within 24 hours of injury six digits (10 percent) required amputation, compared with 97 digits (41 percent) among patients with comparable injuries not treated with tPA • Another single center retrospective study involved 62 patients given thrombolysis with an overall digit salvage rate was 68.6 percent • A smaller single center retrospective study of 13 patients given thrombolysis showed a digit salvage rate of 83.4 percent
Wound care • Usual aseptic technique • Let extremities dry after water bath • Non-adherent gauze for first layer • Loose dressings • Blisters: no clear answer • Clear blisters can be drained / debrided. Hemorrhagic blisters can be aspirated but NOT debrided. • Tetanus as needed • No need for prophylactic antibiotics
Complications: Usually due to subsequent neurovascular injury, and altered sympathetic tone • Short term complications • Pain (weeks) • Parasthesias / electrical shock sensation • Hyperhidrosis • Gangrene / infection • Compartment syndrome • Long term complications • Pain / sensory problems / neuropathy • Vasospasm • Hypersensitivity to cold -> increased susceptibility to recurrent cold injury
Prevention • Cold exposure is contraindicated 6 months after minor injury and 12 months after significant injury • Adequate calories and hydration • Avoid alcohol • Appropriate clothing (wicking layer / insulating layer / hard shell) • Remove wet clothing if possible
Primary source • https://www.uptodate.com/contents/frostbite?search=frostbite&source=search_result&selectedTitle=1~44&usage_type=default&display_rank=1