Hereditary Angioedema
Hereditary Angioedema Ianis Bumber, MD, Peyman Borghei, MD, Sandra Groot, MD, Department of Medicine, Good Samaritan Hospital, Baltimore, MD. Images. Discussion

Hereditary Angioedema
E N D
Presentation Transcript
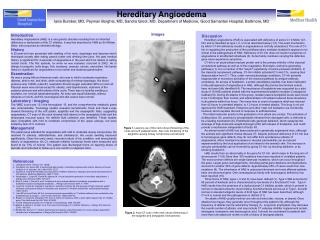
Hereditary Angioedema Ianis Bumber, MD, Peyman Borghei, MD, Sandra Groot, MD, Department of Medicine, Good Samaritan Hospital, Baltimore, MD Images Discussion Hereditary angioedema (HAE) is associated with deficiency of active C1 inhibitor (C1-Inh) and is classified as type I, II, or III as described below (1,2). The exact mechanism by which C1-Inh deficiency results in angioedema is not fully understood. The role of C1-Inh in regulating the production of the proinflammatory mediator bradykinin appears to be critical in the pathogenesis of HAE. Deficiency of C1-Inh does not result in symptoms of angioedema in all affected individuals (3). Some family members carrying the defective gene never experience symptoms. C1-Inh is an acute-phase reactant protein and is the primary inhibitor of the classical complement pathway as well as of the coagulation, fibrinolytic, and kinin-generating pathways (1). It is a member of the "serpin" superfamily of serine protease inhibitors. In the classical complement pathway, C1-Inh inhibits activated C1r and C1s, causing their disassociation from C1. Thus, under normal physiologic conditions, C1-Inh prevents inappropriate or excessive activation of the classical pathway by antigen-antibody complexes. An excess of bradykinin, a potent vasodilatory peptide, has been implicated in the pathogenesis of angioedema in HAE, although the precise biochemical events have not been fully identified (4). The importance of bradykinin was supported by a pilot study of 15 HAE patients treated with the experimental bradykinin receptor-2 antagonist Icatibant (5). During 20 attacks in this group, median plasma bradykinin levels were found to be 7-fold higher than normal, and administration of Icatibant reduced these elevations in all patients within four hours. The mean time to onset of symptom relief was reduced from 42 hours in untreated attacks, to 1.2 hours in treated attacks. This drug is not yet approved for HAE treatment. Histamine and other mast cell mediators are not directly involved, which explains the lack of response to antihistamines. The initial molecular events in the generation of an attack are unclear. The activation of clotting factor XII, possibly by phospholipids released from damaged cells, is believed to be a leading mechanism (6). Endothelial cells generate kallikrein, which catalyzes the cleavage of high-molecular-weight-kininogen (HK) with release of bradykinin, and could provide a mechanism independent of factor XII. An animal model of HAE has been produced in genetically engineered mice, although the animals lack significant clinical disease (7). Despite profound deficiency of C1-Inh due to homozygous gene defects, they do not suffer from spontaneous attacks of angioedema. Minor localized increases in vascular permeability can be induced experimentally by the local application of an irritant to the animal's skin. The increase in vascular permeability can be reversed by giving C1-Inh, by blocking kallikrein, or by blocking bradykinin. HAE results from an abnormality in the gene for C1-Inh, which maps to the long arm of chromosome 11 (8). More than 100 mutations have been reported in unrelated patients. The most common defects are single base-pair mutations, which can occur throughout the gene. Larger gene rearrangements, including partial gene deletions and duplications, account for another 20% of gene defects. Approximately 25% of cases result from new mutations (9). The inheritance of HAE is autosomal dominant and most affected patients have one abnormal gene. One consanguinous family with homozygous deficiency has been reported (10). Three forms of HAE, types I, II and III, have been defined (1). Type I HAE accounts for 85 percent of kindreds and is characterized by low levels of a functional C1-inh. Type II HAE results from the presence of a dysfunctional C1 inhibitor protein, which is present in normal or elevated amounts. Upon testing, functional levels are low as in Type I, but with normal or elevated antigenic levels. A third type of HAE has been described, although C1-inh is normal and the pathogenesis is distinct (11) . An attack of HAE usually involves one site at a time (skin, viscera, or larynx). Once attacks have begun, they generally recur throughout the patient's life, although the frequency of attacks can be reduced by therapy (1). Long-term prophylaxis may decrease the overall number of attacks, and may include C1 esterase inhibitor replacement protein, androgens, tranexamic and aminocaproic acid. It should be considered for patients with more than one attack per month or with a history of laryngeal attacks. Introduction Hereditary Angioedema (HAE) is a rare genetic disorder resulting from an inherited deficiency or dysfunction of the C1 inhibitor. It was first described in 1888 by Sir William Osler, who proposed an inherited etiology. History A 22-year-old man presented with swelling of his neck, dysphagia and dyspnea which developed acutely after eating peanut butter and drinking lime juice. His past medical history is significant for 4 episodes of angioedema in the past which he relates to eating certain foods. The first episode, for which he was intubated, occurred in 2002. He is allergic to propofol, sulfa drugs, fish, tomatoes, peanuts, carrots, and pollen. His family history is significant for angioedema in his mother and maternal grandmother. Examination He was a young African American male, who was in mild to moderate respiratory distress, able to eat and drink, while complaining of minimal dysphagia. His blood pressure was 140/90, pulse 83, respiration 20 and oxygen saturation 98% on room air. Physical exam was normal except for obesity, mild hypertension, erythema of the posterior pharynx and mild edema of the uvula. There was no tonsillar swelling or exudates, nor cervical lymphadenopathy. Air entry was equal bilaterally, without wheezes or ronchi, and the neurological and skin exams were normal. Laboratory / Imaging The WBC count was 13.3 the hemoglobin 15, and the comprehensive metabolic panel was unremarkable. Toxicology studies revealed cannabinoids. Neck and chest x-rays showed thickening of the soft palate, epiglottis and the aryepiglottic folds, suggesting angioedema. CT scan of the neck showed mild edema in the aryepiglotic folds and the pharyngeal mucosal space. No definite fluid collection was identified. These studies were compatible with mild to moderate compromise of the upper airways, but were limited by lack of IV contrast. Management The patient was admitted for angioedema with mild to moderate airway compromise. He received IV steroids, antihistamines, and clindamycin. His uvular swelling improved significantly. Given the early onset, recurrent nature of his condition, and strong family history of angioedema, his C1 esterase inhibitor functional levels were measured and found to be 13% of normal. The patient was discharged home on tapering doses of steroids and instructed to follow up in one month in outpatient clinic. Figure 1. Lateral x-ray of the neck shows thickening of the uvula and soft palate(arrows). Also note thickening of the epiglottis causing airway compromise (arrowhead). • References • UpToDate Online, Version 16.1 (2008) • Donaldson VH, Evans RR. A biochemical abnormality in hereditary angioneurotic edema: Absence of serum inhibitor of c’1-esterase. Am J Med 1963; 35:37. • Agostini A, Cicardi M. Hereditary and acquired C1-inhibitor deficiency: biological and clinical characteristics in 235 patients. Medicine (Baltimore) 1992; 71:206. • Nussberger J, Cugno M, Cicardi M, Agostoni A. A local bradykinin generation in hereditary angioedema. J Allergy Ckun Immunol 1999; 104:1321. • Bork K, Frank J, Grundt B, et al. Treatment of acute edema attacks in herediatary angioedema with a bradykinin receptor-2 antagonist (Icatibant). J Allergy Clin Immunol 2007; 11:1497. • Cugno M, Cicardi M, Coppola R, Agostoni A. Activation of factor XII and cleavage of high molecular weight kininogen during acute attacks in hereditary and acquired C1-inhibitor deficiencies. Immunopharmacology 1996; 33:361. • Han ED et al and Davis AE 3rd. Increased vascular permeability in C1 inhibitor-deficient mice mediated by the bradykinin type 2 receptor. J Clin Invest. 2002 Apr. 109(8):1057-63. • Bissler JJ, Cicardi M, Donaldson VH, et al. A cluster of mutations within a short triplet repeat in the C1 inhibitor gene. Proc Natl Acad Sci USA 1994; 91:9622. • Tosi M. Molecular genetics of C1 inhibitor. Immunobiology 1998; 199:358. • Blanch A, Roche O, Urrutia I, et al. First case of homozygous C1 inhibitor deficiency. J Allergy Clin Immunol 2006; 118:1330. • Binkley KE, Davis A 3rd. Clinical, biochemical and genetic charachterization of a novel estrogen-dependent inherited form of angioedema. J Allergy Ckin Immunol 2000; 106:546. Figure 2. Axial CT-scan of the neck shows thickening of the epiglottis and ariepiglottic folds(arrows).