Download
1 / 32
320 likes | 368 Vues
Explore the principles, impact, and evolution of clinical competency assessment, including tools like OSCE and Mini-CEX. Learn the pros and cons of different assessment scenarios. Enhance your understanding of educational cause and effect in assessment practices.

E N D
Assessment of Clinical Competencies Zubair Amin MD MHPE Associate Professor; Dept of Pediatrics Yong Loo Lin School of Medicine Senior Consultant; Dept of Neonatology National University Hospital
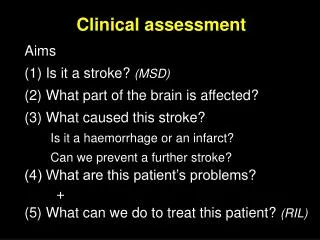
Overview of clinical assessment • Basic psychometric principles on clinical assessment • Bias • Sampling • Context specificity • Basic educational principles about clinical assessment • Educational impact • Feedback • Quality assurance • General properties of innovative instruments
“ Assessment Drives Student Learning.” George E Miller 1919-1998
“Assessment drives learning in at least four ways: its content, its format, its timing and any subsequent feedback given to the examinee.” vander Vleuten, C. (1996) The Assessment of Professional Competence: Developments, Research and Practical Implications, Advances in Health Sciences Education, 1, pp. 41–67.
Professional authenticity Knowledge and Performance Does Shows how Knows how Knows Miller GE. The assessment of clinical skills/competence/performance. Academic Medicine (Supplement) 1990; 65: S63-S7.
Examiner Question
Examiner Question
Examiner Question
Examiner 1 Examiner 2 One student One case: a patient with diabetes mellitus Scenario A 30 minutes for long case Decision: Pass Total Examiners’ Time: 60 minutes (30X2)
Examiner A Examiner B Examiner C Examiner D Diabetes Mellitus Rheumatoid Arthritis Asthma Stroke Scenario B 15 minutes for each long case Decision: Pass Total Examiners’ Time: 60 minutes (15X4)
You are the Chairperson of the examination committee. The particular candidate is known to be weak. In which situation (Scenario A or Scenario B) you are more comfortable in examiners’ decision to pass the candidate? What are the comparative advantages and disadvantages between Scenario A and Scenario B?
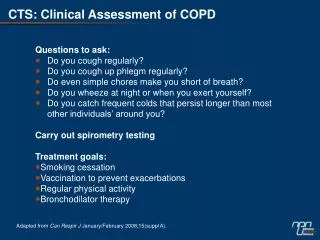
Context Specificity • There is no generic problem solving skills Geoff Norman Management of Diabetes Ketoacidosis = Outpatient management of diabetes Management of COPD = Management of rheumatoid arthritis Diagnosis of asthma = Counseling of asthma patient Typical correlation of “skills” across problems is 0.1 – 0.3
“The ‘law’ of educational cause and effect states that: for every evaluative action, there is an equal (or greater) (and sometimes opposite) educational reaction.” Schuwirth, L.W.T. (2001) General Concerns About Assessment. Web address: www.fdg.unimaas.nl/educ/lambert/ubc “Assessment drives learning in the direction you wish.”
Unintended Consequences of Assessment Evolution of Medical Students Website by NUS students:http://medicus.tk
Educational Impact and Feedback • Any test is anxiety provoking for the students and (staff) • Test has potential positive and negative steering effects on learning and professional development • We tend to assess more, but provide considerably less feedback • Provision for feedback should be strongly considered in performance-based assessment
Concept of Mastery ‘All or none state’ – not really
Continuum of Clinical Competencies Student Trainee Doctor in Practice
A examination that attempts to test students’ competency at a given point of time is less preferable than one that tests the competency over a span of time
Some Common Features in Assessment of Clinical Competency • Multiple examiners • Multiple cases (patients, problems) • Context free • Over a span of time • Feedback and improvement of learning
Traditional Clinical Examination • One/two examiners evaluate a candidate • Candidate takes one patient • Tasks • Take history • Complete physical examination • Interpret data • Generate differential diagnosis • Discuss the patient problem with examiners
Issues • Single patient: context specificity • Single examiner: bias • Patient: mostly in-patients • “Exam” patients • Artificial • Unlike most physician-patient encounters • Limited or no opportunity for observation of communication • Limited or no opportunity for feedback
Instruments for Clinical Competency Assessment • OSCE • Mini-CEX • DOPS • 360 degree evaluation • Portfolio • Many others
Mini-CEX • Assessor observes a trainee in any setting • Takes into account of contexts • Complexity • Focus of visit (diagnosis, management, follow-up) • Uses standard form (not customized to particular patient/problem) • Completes 6-10 encounters
Implementation Issues • Generally reliable and reproducible • At least 4-6 encounters • Different assessors, different patient, different context • Feedback
The mini-clinical evaluation exercise ( mini -CEX) form Norcini, J. J. et. al. Ann Intern Med 2003;138:476-481
Direct Observation of Procedural Skills • Mini-CEX equivalent for procedural skills assessment • Similar psychometric properties • Observation of procedures with real patients • Minimum of 4-6 procedures, different assessors • Provision of feedback
3600 Assessment / Multi-Source Feedback • Involves evaluation of the candidate by multiple individuals within the sphere of influence • Self, superior, peers, co-workers (nurse, ward clerk) • Assessment of professionalism
3600 Assessment • Multiple observations by multiple observers • Over a period of time • Provide evidence, as opposed to impression • Highly valued as a developmental tool
3600 Assessment • Focus on behavior: action taken by the individual • Not used for knowledge or skills • Nurses often are better discriminators • Difficult to standardized grades Unsatisfactory Satisfactory Superior • Customize to your needs
Fundamental Principles • Assessment should be driven by purpose • Consider both psychometric and non-psychometric parameters of assessment tool • Create a backbone of assessment with few high quality, practical tools • Strive towards holistic profiling of a candidate