Download

1 / 10
100 likes | 120 Vues
Professor Daniel Steenstra, Royal Academy of Engineering Visiting Professor in Medical Innovation at Cranfield University, discusses his work on disruptive innovation in healthcare, exploring topics such as diagnostic ultrasound, augmented reality for surgical procedures, genetic therapies, and whole-system transformation. He shares observations on the challenges of adoption and diffusion, the disconnect between technology push and user pull, and the lack of design thinking and stakeholder involvement in the public sector. He emphasizes the need for a shift towards enabling technologies, embedding design principles, and political engagement for transformative change in healthcare.

E N D
The Long and Winding Road to Adoption Professor Daniel Steenstra Royal Academy of Engineering Visiting Professor in Medical Innovation at Cranfield University • A Living Architecture for Transformative Change in Healthcare
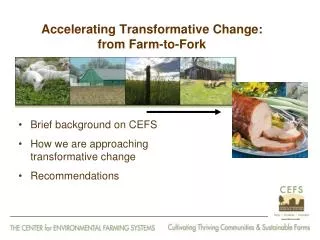
The work I do The two sides of disruptive innovation: • ‘Shop floor’ healthcare innovation - Diagnostic ultrasound in community setting - Augmented Reality for complex surgical procedures - Genetic therapies • Whole system transformation of health care
My observations and insights • Adoption and diffusion is hit & miss especially if provider has to pay and implement This applies across the board – medical devices; drugs and Health 2.0 products • Too much technology push; not enough pull Technology itself is straightforward – lots of people are capable to develop effective solutions ‘Warehouse’ of great technologies not being used • The ‘layered consumer’ User ≠ payer ≠ beneficiary • Patients do not behave like consumers
Whole system breakdown • Lack of design-thinking of large public sector provider No design means no vision no leadership no innovation no user focus • Political control rather than enabling • Not all stakeholders involved
Whither Health2.0 Health 2.0 as enabling technology for: • medical process • core medical technologies • health and social care processes
5 Rules • Own the area - fully understand the domain – e.g. clinical syndrome; current pathway; reimbursement • Differentiate between who pays for the product; who is going to use it and who benefits • Determine who are all the stakeholders and involve them throughout development • Apply design principles – co-design; early prototyping • Pre-empt all aspects of implementation Be patient; find friends with deep pockets; get a hobby or consider doing something else
Solutions for whole system • Political disengagement; from control to enabling • Embed design including associated aspects such as leadership, vision, innovation