Immediate vs. Delayed Angioplasty in Non-ST Elevation ACS: A Randomized Trial
This multicenter randomized trial investigates whether an immediate invasive strategy (primary PCI) is superior to a delayed intervention (next-day strategy) for patients with moderate-to-high risk non-ST elevation acute coronary syndromes (NSTE-ACS). Although the immediate approach is feasible, it does not significantly reduce myocardial infarction rates or affect other efficacy or safety outcomes compared to the delayed strategy. However, it notably shortens hospital stays, suggesting practicality in certain clinical contexts. The study is funded by the French Ministry of Health.

Immediate vs. Delayed Angioplasty in Non-ST Elevation ACS: A Randomized Trial
E N D
Presentation Transcript
Angioplasty to Blunt the rise Of troponin in Acute coronary syndromes Randomized for an immediate or Delayed intervention A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in Patients with Non-ST Elevation ACS G. Montalescot, on behalf of the ABOARD investigators Funded by the Programme Hospitalier de Recherche Clinique (French Ministry of Health) Sponsored by Assistance Publique-Hopitaux de Paris (AP-HP) Led by the A.C.T.I.O.N. group (Academic Research Organization) Coordinating Center: Pitié-Salpêtrière University Hospital Data Management and Statistics: URC Lariboisière University Hospital Additional support from Eli-Lilly G. Montalescot, disclosure: research grant, consulting or speaker fee from BMS, Boston scientific, Cordis, Daiichi Sankyo, Eli Lilly, GSK, SAG, MSD, The Medicines Company, Medtronic, Novartis, Portola, Schering.
Background • Randomized trials have demonstrated that an invasive strategy is superior to a conservative strategy in NSTE-ACS • The optimal timing of intervention remains a matter of debate • A “primary PCI” approach of NSTE-ACS has not been tested yet
Study objective To determine whether immediate intervention (“primary PCI strategy”) is superior to delayed intervention (“next day strategy”) in patients with moderate-to-high risk (TIMI score > 3) non-ST segment elevation ACS.
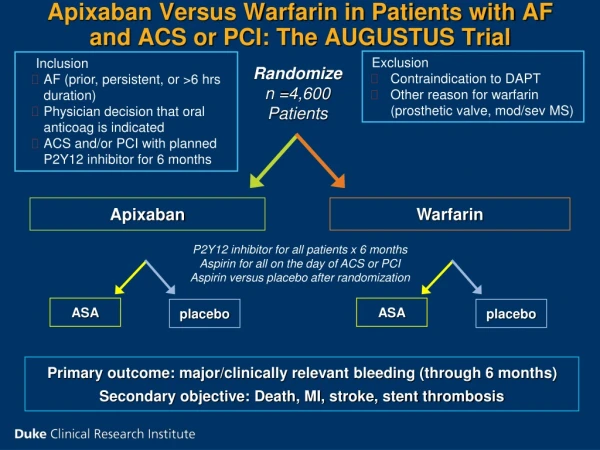
ABOARD study design NSTE-ACS 2 of 3 Criteria: Ischemic symptom, ST-T change, troponin rise with TIMI score > 3 IVRS RANDOMIZATION Next day cath Immediate cath All PCIs on abciximab 1-month Follow-up
ACS Antman EM et al – NEJM 1996 Nienhuis MB et al - CCI 2008 1.35 (1.13-1.60) ALL PCI Troponin during hospitalization « The preferred biomarker for myocardial necrosis is cardiac troponin »
Outcomes Primary MI: defined as the peak of troponin I during hodpitalization Secondary Death (any), new MI (CK-MB) or urgent revascularization (PCI or CABG) Death, new MI, urgent revascularization or recurrent ischemia Individual parameters
Statistical Analysis Study Power: 352 patients: 80% power to detect an effect size equal to 0.3 Randomization: Central 24 hour IVRS Analysis: Intention to treat; Tests: Mann-Whitney test for non-gaussian quantitative parameters, Chi-square or Fisher’s exact probability tests for qualitative parameters . Follow-up: 100%
Peak values of troponin I in the 2 groups Median, IQR 2.1 (0.3-7.1) 1.7 (0.3-7.2) p = 0.70 Primary EP (peak of troponin I)
% P=0.94 P=0.31 Key secondary EP Composite Ischemic Endpoints at 1 month
% P=0.08 P=0.09 P=0.32 P=0.57 P=0.28 P=0.62 Individual Ischemic Endpoints at 1 month
Sites of Major Bleedings n One patient had 2 bleeding events
Median differences and Hodges-Lehmann CI for the primary end point (peak of troponin) Immediate better Delayed better Subgroup analysis (primary EP)
Hospital stay P<0.001
Conclusions A « primary PCI strategy » in NSTE-ACS (compared with a rapid intervention on the next day): • is feasible, but does not reduce the risk of MI (primary outcome) • is not associated with significant differences in other efficacy or safety outcomes • does not benefit to a particular subgroup of patients • shortens significantly hospital stay