IONTOPHORESIS
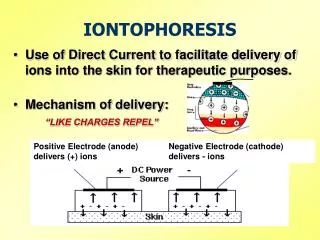
IONTOPHORESIS. Use of Direct Current to facilitate delivery of ions into the skin for therapeutic purposes. Mechanism of delivery: “LIKE CHARGES REPEL”. Positive Electrode (anode) delivers (+) ions. Negative Electrode (cathode) delivers - ions. Historical Highlights.

IONTOPHORESIS
E N D
Presentation Transcript
IONTOPHORESIS • Use of Direct Current to facilitate delivery of ions into the skin for therapeutic purposes. • Mechanism of delivery: “LIKE CHARGES REPEL” Positive Electrode (anode) delivers (+) ions Negative Electrode (cathode) delivers - ions
Historical Highlights • Concept first developed & researched over a century ago. • Therapeutic use for more than 70 years. • Popularity & usage was declining until Joseph Kahn PhD,PT had 9 publications from 1973 to 1983. • Most case studies & clinical commentariesKahn, J. Case Report: Lithium lontophoresis for Gouty Arthritis. J Orthop Sports PhysTher1982;4(2):113-114.
Contemporary Use • In PT: primarily for treating localized inflammatory conditions in superficial tissues • Use corticosteroids, (usually dexamethasone) • Multiple uses of other non-steroidal ions both within & outside PT • Ex: Dentistry, Dermatology, Emergency Dept, Ophthalmology
Ionto: Advantages over injection • non-invasive; less risk of infection • less pain & anxiety • less drug into systemic circulation; decreased side effects • Less risk of local collagen catabolism* * assuming use of corticosteroid
Ionto: Advantages over drug PO • avoids “first-pass” elimination by liver. • less drug into systemic circulation; decreased side effects. • potentially greater concentration of drug in the target area • supervised; maximizes compliance.
Ionto: Disadvantages • risk skin irritation or burn • depth of penetration known to vary b/c of variation of current density, skin impedence, skin/fat thickness, and ionization/pH • greater risk of local collagen catabolism than oral administration* • Action of drug – localized immunosuppression* * assuming use of corticosteroid
Treatment Parameters(when using a DC stimulator eg. “dose controller”) • Current: DC; “high current, short duration” • Amplitude: 0.5 to 4.0 mA is the range • depends on pt. tolerance, polarity, electrode size • Dosage: 40 to 80 mA-min • Dosage Formula: amplitude X time = mA min • Time: calculated by the unit, you set the dosage • The dispersive pad should be put about 6 inches away from the active pad on the same side of the body.
Parameters cont. . . • Polarity – use the same polarity as the drug ion • Rx frequency: every other day at the most • steroid effects can be delayed & last several days • allows time for skin to recover • minimize risk of side effects • cost effective • Rx number: 4 - 7 max • More than 7 treatments in a short period of time can produce detrimental effects such as skin and connective tissue break-down.
Parameters cont. . . • Due to continuous stim using DC, no need for dealing with: • Waveform • Ramp-surge • Frequency • Width • Amplitude, Time, & Polarity abide
Treatment Guidelines (Skin Safety) • Amplitude: the patient feels a slight tingling, itching or mild stinging. Check the skin under both electrodes after ~ 5 minutes. • Mildly red skin under the electrodes is a normal reaction due to vasodilation & heat buildup. • DC can cause mast cells to release histamine = small bumps/vesicles and maybe petechiae. These reactions are normal and resolve within hours. • If the skin is bright red or if many small vesicles are forming, should decrease the amplitude and check skin again after a few minutes. In some cases, may terminate
Many factors affect skin reaction • The patient's skin type & sensitivity to DC current • Current density: not > 0.5 mA/cm2 • Heat build-up; Chemical build-up • Skin pigmentation: skin response harder to judge.
Skin safety cont.. • Caution you about increasing the amplitude after accommodation occurs. • Counterbalance with repeated skin checks • Some clinicians end the treatment by application of a skin lotion containing lanolin or aloe vera.
Contraindications & Precautions • E-stim standard contraindications & precautions apply • Pt. allergic to ions/drugs • Impaired skin sensation is a precaution • No thermal modalities immediately before or after. Why?? • No conductive gel before Ionto. Why?? • Diabetes is a precaution due to decreased peripheral sensation and secondary to localized immunosuppression caused by corticosteroid.
Most Common Ion in PT • Dexamethasone Sodium Phosphate • 0.4% aqueous solution • 0.4% = 0.004 g/ml = 4 mg/ml • corticosteroid for anti-inflammatory • effects; polarity is (-)
Additional Ions(know name, polarity, usage) • Acetic Acid (-) dissolve Ca deposits • Calcium Chloride (+) ms. relaxant • Hyaluronidase (+) disperse edema; not acute • Iodine (-) softens adhesions & scar tissue • Magnesium Sulfate (+) ms. relaxant • Sodium Salicylate (-) ms. & joint pain • Lidocaine (+) local anesthetic • Example pharmacy services
Equipment & Supplies • Drug ion dissolved in aqueous solution or suspended in ointment • Absorbent & buffered electrode • Iontophoresis devices • Dupel DC stimulator by EMPI is what we will use • Numerous other brands of DC stimulators exist • Patch products: Iontopatch, ActionPatch • Newest – Hybresis by EMPI
Patch (Integrated) Systems • Current: DC, “low current, long duration” • Amplitude: ~0.2 mA and less (if constant voltage) • Dosage: 40 to 80 mA-min • more convenient for clinicians and perhaps patients because in-clinic wear time is greatly decreased. Efficacy??
Effectiveness Factors • Dosage: mA-min • Little evidence exists that different combinations of amplitude & duration provide equivalent amounts of ion transfer; some evidence that 4mA X 10 min is best. 40 mAmin is a commonly accepted standard. • Preparation of skin • must be clean; no competing ions. • Depth of target tissue • skin thickness, fat layer, overlying tissues • Electrode Contact
Depth of ion penetration • Believed to occur primarily thru pores (sweat & oil) & hair follicles • Passsive diffusion and local circulation are required to shuttle the drug deeper, to the cells of the target tissue • Research – effect is often inferred based on clinical effectiveness (pain, ROM, MMT, function) • max depth of ion penetration is largely unknown in humans (8-10mm in mammals)