Download
1 / 26
260 likes | 275 Vues
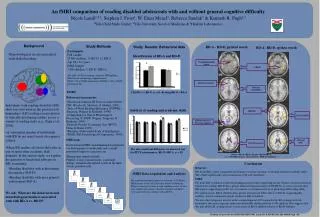
This qualitative observational study explores challenges in transitioning to electronic health records within surgical services. The research sheds light on difficulties faced during the EHR implementation process in surgical specialties. Key findings reveal issues with surgery scheduling, Epic system usability, and sharing clinical responsibilities. The study aims to inform healthcare providers and administrators on improving training and preparation for EHR transitions in surgical practices.

E N D
Challenges of Electronic Health Record Transition for Surgical Services: A Qualitative Observational Study of “Go Live” Megan Shroder Vanderbilt University School of Medicine
Disclosure • I have no relevant relationships with commercial interests to disclose prior to this presentation.
Introduction • Little research has been done about EHR implementations and transitions in surgical specialties, where unique workflows involve transitioning patients from various settings to operating rooms • Most literature about EHR transitions has focused on provider and patient perceptions or simplified process outcomes • Hours spent training • Productivity in patient encounters • Revenue • Patient satisfaction surveys • OR turnover times • Readmission rates • Length of stay • Infection (CLABSI) rates • Mortality • Case volumes • Provider retirement rates
Purpose • We conducted a comprehensive qualitative study to examine the challenges and opportunities in an EHR transition and report preliminary findings from our work in surgical practice settings • This research can inform providers and hospital administrators about the unique challenges to adoption of a new EHR for surgical specialties and opportunities for improved training and preparation
Methods • Large, qualitative, structured observational study using systematic iterative organizational diagnostics • Methodologies were previously utilized to support clinical areas in developing best processes • Observations were done of the Pediatric Surgery inpatient team, OR teams, and outpatient clinics during the transition from a locally-developed EHR (StarPanel) to Epic (Epic Systems Corporation, Verona, WI)
Methods • Informed consent was obtained from providers who were observed on more than one occasion • Facilitated discussion at Surgery Grand Rounds about the recent transition
Methods • Researchers utilized a semi-scripted introduction to the team and then recorded workflows and team interactions • Observations included: • Interactions between providers and other staff or patients • Technologic issues • Workflow interruptions • Work-around techniques developed by the care team
Methods • Representative pictures were taken of messages from hospital administration to staff and error messages related to technology issues • Recurring themes were extracted from the notes of researchers and summarized
Results • Four main categories of issues were identified on surgical services, involving: • Surgery scheduling and coordination with perioperative tests was difficult to navigate and plan • Epic logins, workflows, and functions were anchored to inpatient vs. outpatient settings • Issues often arose when events did not occur on the originally anticipated timeline • Practical ways to share clinical responsibilities within a practice and with trainees was difficult for providers
Results • Surgery scheduling and coordination with perioperative tests: • Orders related to a procedure were often not released until the day of the surgery or were done at an inappropriate time • Teams had difficulty scheduling procedures perioperatively • Critical post-op laboratory and radiographic studies were sometimes lost when encounters for same-day surgery patients were closed • Providers found it difficult to write discharge orders with contingencies
Results • Epic logins, workflows, and functions anchored to binary inpatient vs. outpatient settings: • Attending surgeons and residents work across these settings daily • Many surgeons could not access inpatient information or documentation when working in clinic • Many surgeons encountered problems getting patients from clinic or the ER to the OR for urgent cases • Notes opened in one context could not be signed/attested or were missing key templates, forms, and functions that were available in the other context
Results • Issues arose when events did not occur on the originally anticipated timeline: • Critical orders and post-operative medications were held without notifying the team when patients were not take to the OR as expected • Example: An urgent case was delayed for a more emergent case and was boarded for the next morning. All orders entered by the surgical team were discontinued on the patient overnight without notification
Results • Difficulty sharing clinical responsibilities within a practice and with trainees: • Surgeons were asked to sign orders or board cases while operating • Attending surgeons were unaware of how to attest or co-sign resident orders and notes • There were many requests for attestations or co-signatures that were not previously required or belonged to other attending surgeons • The default for residents was to send attestations to the surgeon with whom they most recently worked (often sent to wrong provider)
Discussion • This study is one of the first comprehensive qualitative studies of an EHR transition to specifically focus on the surgical setting without the use of simplified process outcomes • We identified several themes that have implications for preparation for EHR transition in general and specifically to an Epic system
Discussion • Phases of Care used in the Epic System were a common point of confusion across surgical faculty, residents, and staff • Training for Phases of Care was a limited part of provider education, which was done after the system build and focused on documentation and orders • Activities done in the different Phases of Care in surgery are highly specialty-specific. Workflows varied across surgical specialties and were not amenable to instruction with simple examples • There were numerous help tickets regarding lost orders with several potential patient safety issues, especially when surgery schedules were changed • Changes to the timing of surgeries are incredibly common in organizations that provide trauma care and emergency surgery services
Discussion • The inpatient and outpatient care dichotomy proved challenging for surgical providers who work in both settings each day • The roles and functions of the dichotomy served to be confusing and time consuming for providers • Surgical teams were not well prepared for functioning as group and academic practices (i.e., with support of trainees) • Provider training focused on individual charting responsibilities, with it largely being assumed that the physician provider be consistently available to enter and sign orders • In the emergent setting, surgeons are often busy doing procedures or resuscitating patients • Faculty training did not address how work would be shared among the team
Conclusions • Surgical practices should plan devoted education about the Phases of Care if Epic systems are being implemented • This training should happen early to inform build customization for diverse surgical specialty workflows • Provider education should be focused on how to get patients between various different settings and the OR • Systems with different inpatient, outpatient, and perioperative functionalities are challenging for surgeons to navigate • Dedicated team training should also address sharing clinical work with colleagues, staff, allied health professionals, and trainees in group practice and academic settings
Acknowledgements • Kim Unertl, PhD MS • Shilo Anders, PhD • Laurie Novak, PhD MHSA • Nancy Lorenzi, PhD MA MS • Gretchen Purcell Jackson, MD PhD • This research is covered under: IRB Study 160219 Methods of Organizational Assessment (PI - Laurie Novak) at Vanderbilt University Medical Center • This work was supported by the Research Immersion program at Vanderbilt University School of Medicine, the Surgical Outcomes Center for Kids at Monroe Carell Jr. Children's Hospital, and the Section for Surgical Sciences at Vanderbilt University Medical Center.
Question 1 • Which major theme related to the binary system of inpatient vs. outpatient workspaces was most clearly noticed during our observations of this EHR health transition? • Patients were sometimes seen both on the inpatient and outpatient setting within the same day, making charting for each point of care difficult • Records from inpatient stays were not easy to access or review while seeing a patient in clinic • There were unique processes of writing notes and getting patients to the OR from their current location (floor, ICU, home, clinic, ER) depending on inpatient vs. outpatient context • Medications for inpatient and outpatient settings were listed in each context, but differentiating from inpatient medications and home medications was difficult • The previously utilized EHR was incorporated into both the inpatient and outpatient setting in different ways, making it difficult to access
Question 1 • Which major theme related to the binary system of inpatient vs. outpatient workspaces was most clearly noticed during our observations of this EHR health transition? • Patients were sometimes seen both on the inpatient and outpatient setting within the same day, making charting for each point of care difficult • Records from inpatient stays were not easy to access or review while seeing a patient in clinic • There were unique processes of writing notes and getting patients to the OR from their current location (floor, ICU, home, clinic, ER) depending on inpatient vs. outpatient context • Medications for inpatient and outpatient settings were both listed in each context, but differentiating from inpatient medications and home medications was difficult • The previously utilized EHR was incorporated into both the inpatient and outpatient setting in different ways, making it difficult to access
Explanation • While many of these issues might be true for various EHR transitions and would cause difficulty in caring for patients, C was the correct answer for this question. During our observations, many providers had difficulty charting on inpatient and outpatient settings within the same day because each context had unique note writing activities and functions. • When opening the outpatient view, a provider would have a different view of the patient’s chart than the inpatient view. Providers were also seeing some patients on the inpatient and outpatient setting within the same day and managing their medications for both settings; however, large issues were not observed with this process. Our previous EHR was also available for reference via a fairly accessible link in both the inpatient and outpatient setting.
Question 2 • How were many of the initial problems managed by the surgical staff and healthcare providers within the first week following our EHR implementation? • Personal meetings with EHR experts to redesign the system and fix the problem • Calling a help line with an immediate EHR representative to assist the provider or staff member • Relying on educational materials or literature provided by the hospital administration or EHR staff to solve the issue • Utilizing at-the-elbow staff positioned in each clinical workspace to bypass the issue • Placing help tickets or requests to EHR staff and finding another way to bypass the problem in the short-term
Question 2 • How were many of the initial problems managed by the surgical staff and healthcare providers within the first week following our EHR implementation? • Personal meetings with EHR experts to redesign the system and fix the problem • Calling a help line with an immediate EHR representative to assist the provider or staff member • Relying on educational materials or literature provided by the hospital administration or EHR staff to solve the issue • Utilizing at-the-elbow staff positioned in each clinical workspace to bypass the issue • Placing help tickets or requests to EHR staff and finding another way to bypass the problem in the short-term
Explanation • The correct answer to this question is E. Many of the residents, nursing staff, and attendings were developing their own work-arounds to various issues, such as getting pages sent to their phones when pagers were not working or using written OR whiteboards in the PACU and ORs instead of the malfunctioning electronic versions. • Other issues, such as not being able to print opiate prescriptions for discharge or major patient safety issues were not able to be handled this way and one designated provider would continue calling for help about their placed help tickets from the EHR team until solutions had been found. While there were educational tools provided and at-the-elbow staff available, many of these staff were not familiar with how to problem-solve in our institution-specific design of the EHR and providers stopped utilizing them quickly. • This pattern of innovative solutions and an initial sense of provider dissatisfaction with decreased productivity has also been observed in other EHR transitions, such as the adoption of EPIC at Kaiser Permanente Hawaii in 20037.
Thank you! • megan.m.shroder@vanderbilt.edu
AMIA is the professional home for more than 5,400 informatics professionals, representing frontline clinicians, researchers, public health experts and educators who bring meaning to data, manage information and generate new knowledge across the research and healthcare enterprise. AMIA 2018 Clinical Informatics Conference | amia.org