How to measure cervical length
150 likes | 262 Vues
Learn how to measure cervical length for routine pregnancy care and high-risk patients to assess preterm delivery risk. Understand the ultrasound approach, maternal positioning, and factors affecting accurate measurements.

How to measure cervical length
E N D
Presentation Transcript
How to measure cervical length Karl Oliver Kagan and Jiri Sonek
How to: measure the cervical length Indication: routine pregnancy care and for patients with an increased risk of preterm delivery When?At20–24 weeks’ gestation and anytime in patients with an increased risk of preterm delivery (11–13 weeks) Ultrasound approach: transvaginal or transperineal Ideal maternal position: dorsal lithotomy
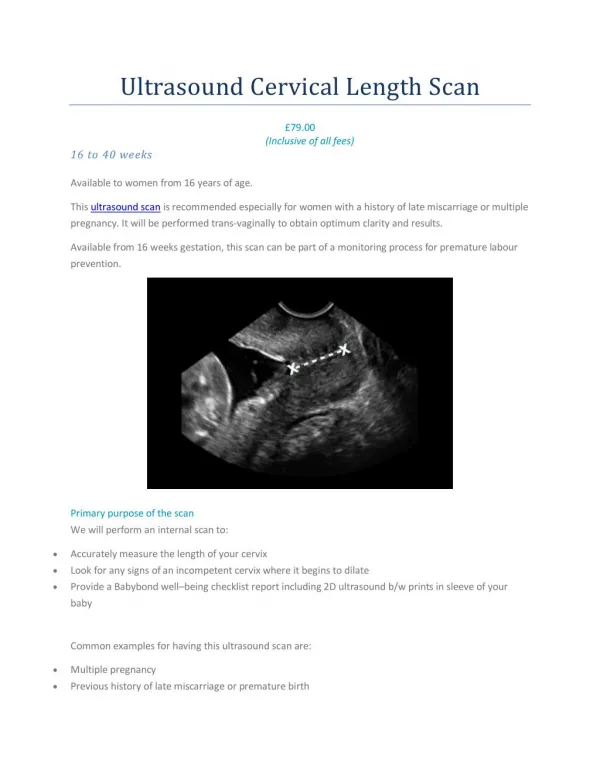
Videoclip S1: Normal.avi The cervix should be measured along its longitudinal axis. The cervix should occupy approximately 50–75% of the image. Excessive pressure on the cervix by the probe should be avoided, as the cervix artificially appears to be longer and the presence of a funnel will be obscured. The examination should last for 3–5min. Several (at least three) measurements should be obtained during the course of the examination and the shortest measurement should be used for counseling.
14mm 27mm Full bladder Empty bladder A full bladder can artificially increase the cervical length. To et al. showed that mean difference between the cervical length measured with an empty and full bladder is about 4mm. In addition, a full bladder can obscure the presence of cervical funneling by compressing the two halves of the funnel together.
The cervical canal and the surrounding cervical mucosa need to be identified.In order to avoid inclusion of the isthmus into the cervical length measurement, care must be taken to identify the internal, as well as the cervical, os. The external cervical os is identified as the point where the anterior and posterior lips of the cervix come together. The identification of the internal cervical os can be more challenging. Identification of the cervical mucosa as a homogenous and hypoechoic structure, compared to the surrounding stroma, can be helpful in these cases, as the internal cervical os is located at the point where the cervical mucosa ends.
cervix isthmus This is particularly important when measuring the cervical length in the first trimester.
Videoclip S2:Ex_pressure.avi Excessive pressure on the cervix by the probe should be avoided, as the cervix artificially appears to be longer and the presence of a funnel will be obscured.
Videoclip S3:Dyn_cervix.mov The cervix is not a static structure and the length can vary, for example due to uterine contractions or a different position of the patient. Therefore, sufficient time should be allowed for the examination to detect these changes. It may be helpful to manually press on the uterus or to ask the patient to push downwards to assess the cervical stability. Some even suggest that the patient stands up during the examination, with the ultrasound probe inside the vagina.
Long curved cervix Short straight cervix If the cervix exceeds 25mm, it will be curved in more than half of the cases. The standard method of measurement, using a straight line between the internal and the external ora, will underestimate the cervical length in these cases. However, this is of little clinical significance as these patients are at low risk regardless of the exact measurement. In the high-risk group of patients with a cervical length < 16mm, the cervix will always be a straight line.
Funneling, defined as protrusion of the amniotic membranes into the cervical canal, is considered by some as an additional risk factor of preterm delivery. Various criteria for the diagnosis of true funneling have been published. However, using a logistic regression analysis that includes both funneling and cervical length, funneling has been shown not to be an independent risk factor.
The cervical canal may have a thin layer of hypoechoic contents. This is especially true in the third trimester. In all likelihood, this represents accumulation of mucus. This finding needs to be differentiated from a thin cervical funnel. This is best done by delineating the course of the fetal membranes: if they are not prolapsing into the cervical canal and are located at the level of the internal cervical os, the presence of a true funnel is unlikely.
Videoclip S4:Sludge.avi Amniotic fluid sludge can be found as echogenic aggregates close to the internal os or within a funnel. This appears to be associated with microbial invasion of the amniotic cavity. Sludge is an independent risk factor for spontaneous preterm delivery, preterm premature rupture of membranes, microbial invasion of the amniotic cavity and histological chorioamnionitis in asymptomatic patients at high risk for spontaneous preterm delivery.
Care should be taken to identify vasa previa (left), placenta previa (right), or a low-lying placenta.
In general, the cervix should be assessed transvaginally. In cases where transvaginal ultrasound should be avoided, such as premature rupture of membranes, the cervical length can be measured by a transperineal approach. The transabdominal assessment of the cervical length can be used as an initial evaluation but a proper risk assessment should be based on a transvaginal or transperineal measurement.