ANTINEOPLASTIC AGENTS
ANTINEOPLASTIC AGENTS. Edited by: Israa Eltayib. Antineoplastic Agents. Antineoplastic medications: drugs used to treat cancer Also called cancer drugs ,cytotoxic agents and anticancer drugs. Cancer. Along with heart disease, cancer is the largest cause of death in the developed world

ANTINEOPLASTIC AGENTS
E N D
Presentation Transcript
ANTINEOPLASTIC AGENTS Edited by: Israa Eltayib
Antineoplastic Agents • Antineoplastic medications: drugs used to treat cancer • Also called cancer drugs ,cytotoxic agents and anticancer drugs.
Cancer • Along with heart disease, cancer is the largest cause of death in the developed world • Cancer affects 1 in 3 people and is responsible for 25% of all deaths • Cancer is an unregulated proliferation of cells due to loss of normal controls, resulting in unregulated growth, lack of differentiation, local tissue invasion, and, often, metastasis. • Cancer can develop in any tissue or organ at any age. There is often an immune response to tumor. • Many cancers are curable if detected at an early stage, and long-term remission is often possible in later stages.
Causes of Cancer • 30 % is due to smoking: lung, mouth, pharynx, larynx, esophagus, urinary bladder, pancreas, and kidney cancers. • Lifestyle – diet, alcohol consumption, reproductive behavior, sexual behavior, exposure to sunlight, etc. 3. At least 15% are related to viruses, e.g. cervical cancer caused by human papillomavirus
Types of Tumors • Benign: non cancerous and not an immediate threat to life, even though treatment eventually may be required for health. • Malignant: tending to worsen and cause death, invasive and metastasis
Characteristics of cancer cells: • Persistent cell proliferation • Invasive growth • Metastases (a tumor may shed cells into the circulation. Although most circulating tumor cells die as a result of intravascular trauma, a tiny number adhere to the vascular endothelium and penetrate into surrounding tissues, generating independent tumors (metastases) at distant sites.)
Etiology of Cancer • Genetics • Viruses • Occupational and Environmental Carcinogens • Radiation
Cont.: Etiology of Cancer • Genetic;mutations are largely responsible for the generation of malignant cells. Two major categories of mutated genes are oncogenes and tumor suppressor genes. • Oncogenes:is a gene that has the potential to cause cancer. • Aproto-oncogene: is a normal gene that regulate cell growth which can become an oncogene due to mutations or increased expression • Mutation of these genes may result in direct and continuous stimulation of the molecular biologic pathways that control cellular growth and division. • For example, the ras gene encodes the Ras protein, which regulates cell division. • Mutations may result in the inappropriate activation of the Ras protein, leading to uncontrolled cell growth and division.
Cont.: Etiology of Cancer • Tumor suppressor genes • are inherent genes that play a role in cell division and DNA repair and are critical for detecting inappropriate growth signals in cells. • If these genes, as a result of inherited or acquired mutations, become unable to function, genetic mutations in other genes can proceed unchecked, leading to neoplastic transformation.
Cont.: Etiology of Cancer • Another important regulatory protein, p53, prevents replication of damaged DNA in normal cells and promotes cell death (apoptosis) in cells with abnormal DNA. • Inactive or altered p53 allows cells with abnormal DNA to survive and divide. • The p53 gene is defective in many human cancers.
Cont.: Etiology of Cancer • Telomeres are nucleoprotein complexes that cap the ends of chromosomes and maintain their integrity. • Telomere shortening occur with aging. • Telomerase is an enzyme that provides for telomere synthesis and maintenance, thus telomerase may potentially allow for cellular immortality. • Telomerase activity may promote tumors through multiple, complex mechanisms, especially by subverting the normal DNA synthetic checkpoints
Cont.: Etiology of Cancer • Viruses: • Contribute to the pathogenesis of human malignancies through the integration of viral genetic elements into the host DNA. • These new genes are expressed by the host; they may affect cell growth or division, or disrupt normal host genes required for control of cell growth and division. • Alternatively, viral infection may result in immune dysfunction, leading to decreased immune surveillance for early tumors. • E.g.:Epstein-Barr, nasopharyngeal carcinoma • -Hepatitis B virus, hepatocellular carcinoma • -HIV Kaposi's sarcoma.
Cont.: Etiology of Cancer • Immune system dysfunction as a result of genetic mutation, acquired disease, aging, or immunosuppressants interferes with normal immune surveillance of early tumors and results in higher rates of cancer. • Known cancer-associated immune disorders include : immune deficiency secondary to immunosuppressants or HIV infection ( Kaposi's sarcoma)& rheumatologic conditions, such as Rheumatoid Arthritis (B-type lymphoma).
Cont.: Etiology of Cancer • Radiation: • Carcinogenesis can result from ionizing radiation and may develop from 2 different mechanisms; • Direct ionization – damages DNA and other molecules can cause direct somatic mutations • Secondary effectors such as oxygen radicals can be formed by interaction with ionizing radiation. Oxygen free radicals can damage and kill cells and also induce mutations.
Pathogenesis of Neoplasia • Cancer development can begin with a brief exposure (hours or days) to a chemical into an activated form and the chemical need not be present ever again. • However, DNA is altered via mutagens including chemical carcinogens, viruses, and radiation. • This mutations is inherited by at least one cell division (initiation).
Pathogenesis of Neoplasia • This mutation lead to activation of proto-oncogene into oncogenes (leading to uncontrolled cell proliferation) and/or inactivation of tumor suppressor genes (leading to resistance to apoptosis.) • Upon exposure to other epigenetic factors (hormones, co- carcinogens, immunosuppressant, which themselves are non carcinogenic) tumor growth is promoted (promotion)
Pathogenesis of Neoplasia • Initiation - point at which an irreversible alteration, usually genetic, is introduced into a target cell. • Initiation: • Is essentially irreversible • Caused only by carcinogenic compounds • Occurs rapidly after carcinogen exposure • Alone does not result in tumor formation
Pathogenesis of Neoplasia • Promotion is the process whereby an initiated tissue or organ develop focal proliferations and it requires the presence of continuous stimulation. • Promotion • reversible • acts only after exposure to an initiating agent • requires repeated administration of a promoter • is not carcinogenic in itself
Etiology and Pathogenesis of NeoplasiaInitiation and Promotion
How long does it take to produce a clinically detectable neoplasm ? • It takes at least 30 population doublings to produce 10 9 cells (about 1 gram in weight) from a single, initial transformed cell. It then takes only about 10 population doublings to produce a neoplasm of 10 12 cells (weight about 1 Kg, which is the maximal size compatible with life).
How long does it take to produce a clinically detectable neoplasm ? • By the time a solid neoplasm is clinically detected, it has already completed a major portion of its life cycle (The latent period before which a neoplasm becomes clinically detectable is quite unpredictably long, usually years).
How long does it take to produce a clinically detectable neoplasm ? • The rate of growth of a neoplasm is determined by the proportion of cells in the growth fraction and the degree of imbalance between cell proliferation and cell loss. In the submicroscopic phases of neoplastic growth most cells are in the proliferative pool (growth fraction). By the time a neoplasm is clinically detectable most cells in a neoplasm are not in the growth fraction. 4. The growth fraction of neoplastic cells has a profound effect on their susceptibility to cancer chemotherapy.
There are three basic treatment possibilities for cancer: surgery, radiotherapy, and chemotherapy. • Some cancers where chemotherapy works very well: • Childhood leukemia • Retinoblastoma • Osteosarcoma • Testicular cancer • Hodgkin’s Disease • Some lymphomas • Some early breast cancers
Cancers that are very difficult to treat with chemotherapeutics (need surgery or radiotherapy first): • Colon • Lung • Late stage breast cancer • Pancreatic cancer (WHY???).
Problems associated with chemotherapy 1-Resistance to chemotherapy • Resistance to chemotherapy may develop by several mechanisms: • Decrease in the amount of drug uptake by cancer cells E.G. Methotrexate • Increase in the amount of drug removed by cancer cells. (Transporters=P-glycoprotein). E.G. Vinblastine ,doxorubicin, bleomycin ,etapsoid…. • Decrease or alteration in target molecule sensitivity – this is caused by mutation in the molecule targeted by the drug E.G. Methotrexate, Mercaptopurine, doxorubicin • Increase in DNA repair ability of the cell via an increased expression of DNA repairing enzymes. E.G. Alkylating agent
2-Toxicity and side Effects of Antineoplastic Agents: • Normal cells in the body that tend to be injured the most due to chemotherapy are those which have a high growth fraction. • Those are bone marrow, GI Tract ,hair follicles, reproductive organs . • Leading to the followings: • Alopecia- hair loss • Myelosuppression-bone marrow suppression • Emetic potential: disruptive to cells in stomach which causes: Nausea/vomiting • Low WBC count- low immunity
3-Treatment-induced tumor • Many anticancer drugs are mutagens and can cause the rise of neoplasm ten or more years after the original cancer was cured.
Cell cycle Scientists have determined that cell cycle can be divided into:. Gap 0 (G0): • There are times when a cell will leave the cycle and quit dividing. • This may be a temporary resting period or more permanent. An example of the latter is a cell that has reached an end stage of development and will no longer divide (e.g. neuron). Gap 1 (G1): • Cells increase in size in Gap 1, produce enzymes needed for DNA synthesis
S Phase: • To produce two similar daughter cells, the complete DNA instructions in the cell must be duplicated. • DNA replication occurs during this S (synthesis) phase. Gap 2 (G2): • It is the gap between DNA synthesis and mitosis, the cell will continue to grow and produce new proteins & RNA. Mitosis (M Phase): • Cell growth and protein production stop at this stage in the cell cycle. • All of the cell's energy is focused on the complex and orderly division into two similar daughter cells.
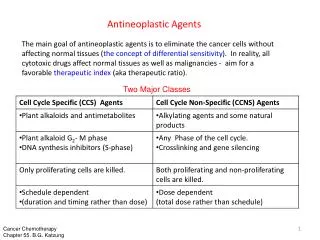
Cancer chemotherapeutic agents They are classified into: • Cell-cycle non specific agents(CCNS): are cytotoxic in any phase of the cycle even on G0 phase and so are more effective against large slowly growing tumors. E.g. Bleomycin. • Cell-cycle specific (CCS): are cytotoxic on all phases but not on cells out of the cycle (at G0 ) and so are more effective against rapidly growing tumors. Work better in combination than alone. E.g. Mitomycin, doxorubicin,….etc. • Phase specific:act on specific phase of the cycle. E.g. Vinca alkaloids act more in M-phase ,antimetabolites (mainly act on S-phase).
Anticancer Drugs There are three Major Groups of Anticancer Drugs: • Cytotoxic Drugs (largest group) • Alkylating agents • Antimetabolites • Antitumor antibiotics • Plant alkaloids • Miscellaneous cytotoxic drugs • Hormones and hormone antagonists • These are among the best-tolerated chemotherapeutics because they target specific receptors, and thus only specific cell types e.g. Tamoxifen • Immunomodulators • Immunostimulants, including interferons and interleukins • Immunosuppressant
I-Alkylating Agents (CCNS) Mechanism of Alkylating Agents • These drugs work by alkylation with nucleophilic substitution . • They alkylate a variety of cellular constituents, such as cell membranes, proteins, and most importantly DNA. More specifically, the nitrogenous bases of DNA are what get alkylated.
The drugs start off as pro-drugs that become activated when a chlorine atom is extracted. • A carbonium ion is thus formed. This “carbonium ion” is very electrophilic and will then attack any free pair of electrons (i.e. on the N7 of guanine). This electrophilic attack results in a bond being formed between the drug and the guanine of DNA. As a result of this “alkylation”, there are a few consequences: 1) Miscoding (In transcription) 2) Cross linking- this only occurs if the drug is bifunctional
Subgroups of Alkylating Agents 1) Nitrogen mustards 2) Nitrosoureas 3) Alkyl sulfonates 4) 4-Platinum Coordination Compounds
1-Nitrogen Mustards • Similar to mustard gas • E.g.: Mechlorethamine, cyclophosphamid, melphalan & chlorambucil A-Mechlorethamine • First alkylating agent employed clinically • Bifunctional, thus can crosslink DNA • Extremely unstable and is inactivated within a few minutes following administration. Thus it is given IV. Clinical Uses • Hodgkin’s Disease • Non-Hodgkin’s Lymphoma Toxicity/ Side Effects • Dose limiting toxicity is bone marrow depression • Nausea/ Vomiting, Diarrhea, Alopecia, Sterility
B-Cyclophsphamid • It acts as cytotoxic and immunosuppressor agent. • Prodrug which must be activated by the cytochrome p450 system, which turns it into a nitrogen mustard. • Bifunctional agent • Most widely used alkylating agent Clinical Uses • Hodgkin’s Disease • Non-Hodgkin’s lymphoma • Solid tumors of head, neck, ovaries, and breast • Frequently used in combination with methotrexate (anti-metabolite) or doxorubicin (anti-tumor antibiotic), or fluorouracil as adjuvant therapy post breast cancer surgery • Organ transplant recipients (due to immunosuppressive actions)
Toxicity/ Side Effects • Bone marrow depression • Severe nausea and vomiting • Acute hemorrhagic cystitis and renal damage?? (Can be minimized via high fluid intake/infusion and the use of………?) • Sterility • Hypersensitivity reactions
2-Nitrosoureas • Bifunctional • Active against broad spectrum of neoplastic disease • Inhibits synthesis of both DNA and RNA, as well as proteins • These drugs are highly lipophilic, so they can easily cross blood-brain-barrier, and are great for CNS tumors. • Big problem in this class is that they are highly mutagenic and highly carcinogenic. • Major toxicity is delayed bone marrow depression & pulmonary fibrosis.
Clinical uses • Primary and metastasis tumors of the brain • Hodgkin’s disease • Non-hodgkin’s lymphoma • Adenocarcinoma of stomach, colon, and rectal cancer • Hepatocarcinoma E.g.: • Carmustine • Lomustine
3-Alkyl Sulfonates • Busulfan Clinical uses • Great effect on Chronic granulocytic Leukemia Toxicity/ Side Effects • Dose limiting toxicity is bone marrow depression. • Pulmonary infiltrates and pulmonary fibrosis • Tonic-clonic seizures in epileptics • Nausea and vomiting • Alopecia • Sterility • Skin hyper pigmentation • Cataracts • Hepatitis
4-Platinum Coordination Compounds E.g.: Cisplatin • Forms crosslinks within DNA strands. • Cis-platin is not really an “alkylating” agent, but since it operates via the same mechanism as the alkylating agents, it is placed within that group. Clinical Uses • Very powerful against TESTICULAR CANCER • Also good for carcinomas of ovary, bladder, head, and neck Toxicity/ Side Effects • Renal tubular damage (minimized via massive hydration coupled with anti-emetics) • Ototoxicity and peripheral neuropathy • VERY SEVER vomiting ( ndanosetron) Carboplatin: is a derivative of cisplatin with less nephero- ,neuro- & ototoxicity.
II-Antimetabolites (CCS) An antimetabolite is a chemical with a similar structure to a metabolite required for normal biochemical reactions, yet different enough to interfere with the normal functions of cells, including cell division. All antimetabolites are used in cancer treatment, as they interfere with DNA production and therefore cell division and the growth of tumors (mainly in S-phase specific). They are classified into: 1- Folic acid analogues 2- Purine analogues 3- Pyrimidine analogues