Download

1 / 43
470 likes | 1.11k Vues
RESPIRATORY DISTRESS IN NEWBORN PART 3. KIRANJIT KAUR. PNEUMOTHORAX. presence of air or gas in the pleural cavity between the visceral and parietal pleura, which results in violation of the pleural space. This causes pressure within the pulmonary space to exceed extrapleural pressure.

E N D
RESPIRATORY DISTRESS IN NEWBORN PART 3 KIRANJIT KAUR
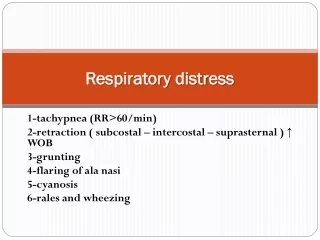
PNEUMOTHORAX • presence of air or gas in the pleural cavity between the visceral and parietal pleura, which results in violation of the pleural space. • This causes pressure within the pulmonary space to exceed extrapleural pressure. • It can occur spontaneously or as a result of infection, meconium aspiration, lung deformity, or ventilation barotrauma. • Frequency : 1-2% in term births 6% in premature births
a.Place light source (otoscope, transilluminator) on infant’s chest. Ensure it isn’t hot. b.A normal chest will have a small glowing “Halo” around the light source. Usually it extends less than 1 cm from the light source and is symmetric. c.If the chest “lights up like a jack-o-lantern or ET’s chest” (large area of redness that is often asymmetric), then ptx should be HIGH on your DDx list. d.You should compare to the other side if you are unsure.
MANAGEMENT • Observation should be the treatment of choice for primary spontaneous small closed pneumothoraces without significant breathlessness, in a spontaneously breathing patient. Inhalation of high concentrations of oxygen may speed the resolution of a pneumothorax by reducing the partial pressure of nitrogen in the pulmonary capillaries. • Aspiration • Chest tube • SpO2 monitoring
ASPIRATION • Equipment • i.Angiocath or butterfly needle (for neonates) • ii.Large syringe (>20mL) • iii.3-way stop-cock (to keep system closed) • Procedure • i.Locate 2nd or 3rd intercostal space at the midclavicular line • ii.Prep skin with antiseptic and provide analgesic/anesthetic. • iii.Advance needle perpendicularly over superior border of rib while aspirating. Having saline in syringe will allow you to detect when you’ve entered the ptx. • iv.When bubbles are present or you have free movement of the syringe plunger, evacuate the pneumothorax. • v.A 3-way stopcock can be placed between syringe and butterfly needle, which will allow for controlled evacuation of pneumothorax.
PERSISTENT PULMONARY HYPERTENSION OF NEWBORN • defined as a failure of normal pulmonary vasculature relaxation at or shortly after birth • Resulting in impedence to pulmonary blood flow which exceeds systemic vascular resistance that unoxygenated blood is shunted to systemic circulation • Data suggest that 2-6 cases of PPHN occur per 1000 live births.
PATHOPHYSIOLOGY • While a fetus is in the womb, it gets its oxygen from its mother's placenta through the umbilical cords, so the lungs need little blood supply. There is high blood pressure in the lungs, so blood in the pulmonary artery is sent away from the lungs to the other organs through a fetal blood vessel, called the ductusarteriosus. • When a baby is born and takes its first breaths, the blood pressure in their lungs falls and there is an increased blood flow to the lungs, where oxygen and carbon dioxide are exchanged. The blood is then returned to the heart and pumped back out to the body. The ductusarteriosus constricts and permanently closes in the first day of life. However, in babies with PPHN, the pressure in the lungs remains high and the ductusarterious remains open, allowing blood to be directed away from the lungs.
Meconium aspiration. Serial radiographs in a newborn with uncomplicated meconium aspiration. Radiograph obtained shortly after birth shows ill-defined, predominantly perihilar opacities in the lungs; these are more severe on the right than on the left. The lungs are hyperexpanded. The neonate's heart size is within normal limits. The abnormalities on the initial chest radiograph, aside from the presence of an endotracheal tube and an umbilical artery catheter, are identical to those seen in severe cases of transient tachypnea of the newborn.
DIAGNOSIS • Chest X-rays may be recommended and can determine if the baby has lung disease or an enlarged heart. • Echocardiogram, which is an ultrasound of the heart, can show whether the baby has heart or lung disease and evaluate blood flow in those organs. • Ultrasound of the head may be used to look for bleeding in the brain. • Arterial blood gas (ABG) determines how well oxygen is being delivered to the body. • Complete blood count (CBC) measures the number of oxygen-carrying red blood cells, white blood cells and platelets. • Serum electrolyte tests evaluate the balance of minerals in the blood. • Pulse oximetry
TREATMENT • Oxygen -- 100 percent supplemental oxygen may be given to your baby through a mask or plastic hood. • Assisted Ventilation -- During this procedure, a tube is inserted into your baby's windpipe and a ventilator takes over your baby's breathing and oxygen is given. • Nitric Oxide -- Research has shown that this gas is effective in treating PPHN because it relaxes contracted lung blood vessels and improves blood flow to the lungs. It is given through the ventilator. • High Frequency Oscillatory Ventilation -- This type of ventilation may improve the oxygen level in the blood if other types of ventilation are not effective. • Extracorporeal Membrane Oxygenation -- In addition, an extracorporeal membrane oxygenation (ECMO) machine may be used for patients who are experiencing serious heart or lung failure. It delivers oxygen to the brain and body as temporary support while the PPHN resolves. ECMO is similar to a heart-lung bypass machine, which takes over your baby's heart and lung functions with an external pump and oxygenator. Blood is drained from the patient to an artificial lung, where oxygen is added and carbon dioxide is removed, and then the blood is pumped back into your child.
1. Blood is drained out of the body through a vein into the ECMO machine, which removes carbon dioxide and adds oxygen allowing the heart and lungs to rest 2. Blood is warmed before being returned to the heart - flow of blood out of the body is steadily reduced as patient recovers
Inotropic drugs-dopamine, dobutamine, and/or milrinone is frequently helpful in maintaining adequate cardiac output and systemic blood pressure while avoiding excessive volume administration. • Surfactant administration • Acidosis and alkalosis correction • Treating hypothermia,hypocalcemia, hypoglycemia
PROGNOSIS • Periods of inadequate oxygenation can have long-term effects on infants who survive PPHN, such as bronchopulmonary dysplasia (a chronic lung disease associated with scarred, stiffened lungs) and breathing difficulties. Seizure disorders, developmental delay, and neurological deficits may also be seen. • Medical treatments such as high frequency ventilation, nitric oxide, and ECMO have significantly decreased the percentage of children who die from PPHN. Fifteen years ago, almost half of infants diagnosed with PPHN died; today, less than 20% of infants with PPHN die, and only about one fifth of surviving infants experience long-term physical or developmental complications.
CONGENITAL DIAPHRAGMATIC HERNIA • is when there is an absence of a child's diaphragm, or a hole in the diaphragm. • This can occur on either the left or right side, but is most common on the left. • The contents the child's abdomen, including stomach, intestines, liver and spleen may go through the hole and into the chest. • This prevents the normal development of the lung on that side, and may affect the growth of the other lung.
TYPES • There are 3 types of diaphragmatic hernia: • Bochdalek hernia: This type involves an opening on the back side of the diaphragm. The stomach, intestines and liver or spleen usually move up into the chest cavity. (left-sided hernia is the most common). occurs in approximately 1 per 3000 live births, more commonly in males • Morgagni hernia: This type is rare and involves an opening in the front of the diaphragm, just behind the breastbone (right-sided hernias, only the liver and a portion of the large bowel tend to herniate.) • Bilateral hernias are uncommon and usually fatal
Chest radiography revealed an enlarged right mediastinum with air content on the right side (Panel A, arrow; and Panel B, lateral view). Thoracic computed tomographic (CT) scans showed a Morgagni's hernia, characterized by an anteromedial diaphragmatic defect, with herniation of the transverse colon and part of the omentum into the thorax (Panels C and D).
SIGNS & SYMPTOMS Symptoms (of a Bochdalek diaphragmatic hernia): • difficulty breathing • tachypnea • tachycardia • cyanosis • abnormal chest development, with one side being larger than the other • abdomen that appears caved in(scaphoid) • In left-sided posterolateral hernia, auscultation of the lungs reveals poor air entry on the left, with a shift of cardiac sounds over the right chest. • Associated anomalies occur in a relatively high percentage of infants. Dysmorphisms such as craniofacial, extremity abnormalities, or spinal dysraphism • A baby born with a Morgagni hernia may or may not show any symptoms.
DIAGNOSIS • During pregnancy : During routine prenatal care at around 18 weeks, an ultrasound may reveal the existence of a diaphragmatic hernia, or what is suspected to be CDH. 2) After birth : After birth, your baby's physician will perform a physical examination. The following tests may also be done: • A chest x-ray is done to look at the abnormalities of the lungs, diaphragm and intestine. • Arterial blood gas is often performed to evaluate the baby's breathing ability. • A blood test for chromosomes helps determine if there is a genetic problem. • An ultrasound of the heart (echocardiogram) provides further details about the child's condition.
TREATMENT • In the delivery room, if the infant is known or suspected to have congenital diaphragmatic hernia, immediately place a vented orogastric tube and connect it to continuous suction to prevent bowel distension and further lung compression. • avoid mask ventilation and immediately intubate the trachea. • Mechanical ventilation strategies are targeted at avoiding high peak inspiratory pressures and synchronizing ventilation with the infant's respiratory effort. • ECMO is a heart and lung bypass system that does the job that the heart and lungs would be doing; ECMO may be used temporarily while the baby's condition stabilizes and improves. • Surgery - When the baby's condition has improved, the diaphragmatic hernia will be repaired with an operation. • The stomach, intestine and other abdominal organs are moved from the chest cavity back to the abdominal cavity. The hole in the diaphragm is repaired, or if the diaphragm is absent, an artificial diaphragm will be constructed.
Thank you for your attention! No questions right…