Download
1 / 50
530 likes | 1.21k Vues
Anxiolytic, Sedative-Hypnotic Drugs Liming Zhou ( 周黎明) Department of pharmacology. Contents. Overview History Benzodiazepines Barbiturates Other drugs. Definitions. Anxiolytic Sedation Hypnosis. The Scream (Edvard Munch, 1893).

E N D
Anxiolytic, Sedative-Hypnotic DrugsLiming Zhou (周黎明)Department of pharmacology
Contents Overview History Benzodiazepines Barbiturates Other drugs
Definitions • Anxiolytic • Sedation • Hypnosis
The Scream (Edvard Munch, 1893) Anxiety (Edvard Munch, 1894)
Anxiety • Feeling of helplessness • Difficulty in concentrating • Irritability & insomnia • GI disturbances • Muscle tension • Excessive perspiration • Palpitations • Dry mouth • Impending doom • Dread(terror)
Clinical Disorders • Panic disorder • Obsessive-compulsive disorder • Post-traumatic stress disorder • Social phobia • Social anxiety disorder • Generalized anxiety disorder • Specific phobia
Sedation • Character: Decreased anxiety Decreased motor activity Decreased mental acuity
Hypnosis • Character: Increased tendency to sleep Induce the soporific state( Sleep)
History • From time immemorial, human beings use of substances that induce behavioral depression to relief anxiety and insomnia. • Both alcohol and opium alkaloids, such as morphine, have been used by individuals to induce a soporific state. • In the latter part of 19th century, bromide and chloral hydrate were developed. • by 1912 Phenobarbital (barbiturate) and within the next 25 years, 50 similar drugs were discovered. • In the1950’s meprobamate was discovered.
History • In 1960, the first receptor-specific drugs, the benzodiazepines was discovered • By the mid 1990’s, non-benzodiazepines, with hopefully fewer side effects and a lower risk for dependence, such as buspirone (Buspar), an anxiolytic and zolpidem (Ambien) a hypnotic were developed. • Presently, the search continues for more effective and safer agents.
Classification 1.Benzodiazepines 2.Barbiturates 3.Other drugs
Benzodiazepines • Pharmacological effects • Mechanism of action • Therapeutic uses • Pharmacokinetics • Adverse effects • Precautions
Pharmacological effects • 1) Reduction of anxiety -At low doses, the drugs cause little sedation -Inhibiting neuronal circuits in the limbic system of the brain selectively
Pharmacological effects • 2) Sedative - Decreased anxiety leads to calming effect - No effects on motor or mental functions - Minimal CNS depression
Pharmacological effect • 3) Hypnotic action -at high doses, produce drowsiness & sleep - higher CNS depression by increased dose
Pharmacological effects • 4) Anticonvulsant -Can exert anticonvulsant effects without marked central nervous system depression, so that mental and physiologic activity are relatively unaffected.
5)Muscle relaxant - Increasing presynaptic inhibition in the spinal cord -Diazepam exert inhibitory effects on polysynaptic reflexes and internuncial transmission and at high doses may also depress transmission at the skeletal neuromuscular junction
Mechanism of Action • “Most” sedative-hypnotics exert effects on GABA A receptor • GABA - the major inhibitory NT in the CNS • GABAa receptors - heteromultimeric structure • 5 transmembrane polypeptide subunits per receptor/channel complex • ,,,,, polypeptide subtypes • Multiple isoforms for each (e.g. 1-6)
Mechanism of Action • GABA binding stimulates Cl- current - hyperpolarizing effect - inhibitory effect on neuronal excitability
Mechanism of Action • GABAA receptor composition varies in different regions • BNZs bind to receptors with alpha & gamma subunits. • BNZ binding “enhances” the effect of GABA on the Cl-channel • BNZs exert no effect in the absence of GABA
Mechanism of action • Bind to benzodiazepine receptor of the GABAa receptor-chloride channel complex • Leads to increased frequency of Cl- channel opening and Cl- conductance • Facilitate GABA-mediated inhibition of neuronal activity, particularly in limbic and cortical areas of CNS
Therapeutic uses • 1.For relief anxiety • 2.For insomnia • 3.For treatment of epilepsy and seizure states
Therapeutic uses • 4.For muscle relaxation in specific neuromuscular disorders • 5.For sedation and amnesia before medical and surgical procedures • 6.For control of ethanol or other sedative –hypontics withdraw states
Pharmacokinetics Benzodiazepines Diazepam • A. Absorption: orally. Diazepam crosses the placental barrier and blood-brain barrier • B. Distribution: Diazepam is extensively distributed in the tissue. Diazepam is highly binding to plasma protein • C. Biotransformation: -Hepatic oxidation: long-t1/2, active metabolites • Glucuronidation: short-t1/2, no active metab. • D. Excretion: The water-soluble metabolites of benzodiazepines are excreted mainly via the kidney.
Adverse effects • A Depression of central nervous system: drowsiness, a significant impact on driving ability • B Tolerance; Psychologic & Physiologic dependence,
Tolerance • -Decreased responsiveness to a drug following repeated exposure is a common feature of sedative-hypnotic use. • -It may result in an increase in the dose needed to maintain symptomatic improvement or to promote sleep.
The reason of tolerance • -The mechanisms responsible for tolerance to sedative-hypnotics are not well understood. • -In the case of benzodiazepines, the development of tolerance in animals is associated with down regulation of brain benzodiazepine receptors.
Precautions • Enhance the effect of alcohol and other CNS depressants • Be care for patients of liver diseases • (why?)
Barbiturates Overview • The barbiturates were the typical sedative-hypnotic for treatment of anxiety and insomnia from 1912 to 1960. • they were also associated with suicides, death by accidental ingestion. • dependency and abuse, along with serious interactions with other drugs and alcohol.
Barbiturates • less commonly used due to undesirable side-effects. • -induces psychologic & physical dependence. • –Dose-dependentsedation, hypnosis, general anesthesia,coma,death.
Classification • Long-acting drugs: phenobarbital • Shorting-acting drugs: • Pentobarbital, secobarbital,amobarbital • Ultra-short-acting drugs: thiopental
Pharmacologic effects and clinical uses • 1. Sedation: barbiturates depress the CNS at all levels in a dose-dependent fashion. • 2. Hypnotics: they decrease the amount of time spent in REM sleep. • 3. Anesthesia and administration before anesthetic. • 4. Anticonvulsant: Phenobarbital.
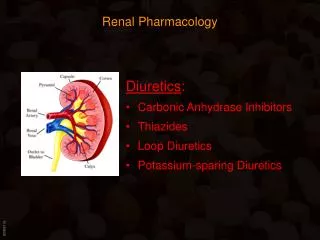
Barbiturates Coma Medullary depression CNS Effects Anesthesia Hypnosis Sedation, Anxiolytics Increasing dose Benzodiazepines Possible selective anticonvulsant & muscle-relaxing activity
Pharmacologic effects and clinical uses • 5. Muscle relaxation • 6. Effects on respiration and Cardiovascular system • 7. Most barbiturates, but especially Phenobarbital, are capable of inducing the hepatic microsomal drug-metabolizing enzyme system(P-450).
Untoward effects • 1.Depressant effects include over-sedation and decrease in REM sleep. • 2. Barbiturate dependence. • 3. Addiction, withdrawal syndrome.
Other drugs • Buspirone • 5-HT-1A mixed agonist-antagonist, weak DA block • Not a benzo, not hypnotic, no tolerance, no dependence, no withdrawal symptoms Anxiolytic, possible efficacy • No anticonvulsant • Start 5 mg t.i.d, max 60 mg/day
It's secreted by the pineal gland, a pea-size structure at the center of the brain. • At night melatonin is produced to help our bodies regulate our sleep-wake cycles. • The amount of it produced by our body seems to lessen as we get older. • This may be can explain why young people have less problem sleeping than older people. Another sedative hypnotic drug • Melatonin (MT)
Melatonin (MT) • Can hasten sleep and ease jet lag, without the hazards or side effects of prescription sleeping pills. • It may have many other uses and has been reported to make people feel better, strengthen the immune system,
Melatonin (MT) • Current research is underway to determine it's effect as an immuno-modulator in cancer, delayed sleep-phase disorders, and jet lag. • Tests are still under way so there is much to still be learned about it and its effects on the human body.
Home work Case study
Case study A 22 yr old woman is brought into the ER via ambulance because of a suicide attempt. Soon after a “night on the town”, she called her boyfriend saying that she took a handful of sleeping tablets. On examination, she appears lethargic, but groans and moves all her extremities to painful stimuli. Her blood pressure is 110/70 mm Hg, heart rate is 80 bpm, and oxygen saturation is 99 percent.
Case Her pupils are of normal size and reactive to light. Her deep tendon reflexes are normal bilaterally. In the field, she was given an intravenous bolus of dextrose and an ampule of naloxone without response. Her boyfriend, with whom she hand an argument, brings in the bottle of sleeping medication which reads “lorazepam”.
Q1: What is the danger of an overdose with this class of medication? Q2: What is the cellular mechanism of action of this class of medication? Q3: What pharmacological agent can be used to treat this patient, and what is its mechanism of action?
2. Description of different point for Benzodiazepines and Barbiturates