Download
1 / 35
350 likes | 719 Vues
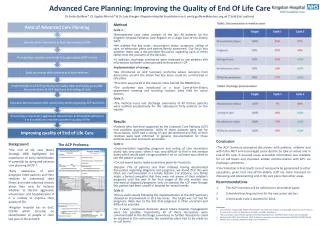
Symposium on Advanced Care Planning. Challenges in executing an Advanced Medical Directives in the local ICU Dr Lim Boon Leng Director, Dept of Intensive Care Medicine Senior Consultant & Deputy Head Dept of Anaesthesia & Surgical Intensive Care Singapore General Hospital.

E N D
Symposium on Advanced Care Planning Challenges in executing an Advanced Medical Directives in the local ICU Dr Lim Boon Leng Director, Dept of Intensive Care Medicine Senior Consultant & Deputy Head Dept of Anaesthesia & Surgical Intensive Care Singapore General Hospital www.anaesthesia.co.inanaesthesia.co.in@gmail.com ®
Intensive Care Unit (ICU) • Specially staffed and equipped hospital ward • Dedicated to management of patients with life- threatening illness, injuries and complications
End-of-life care in the ICU • Our ability to prolong life has advanced dramatically over the years • Aggressive(“heroic”) life support often serves only to prolong the dying process • Many patients die in pain • Few doctors know their patients’ preferences regarding CPR • Despite AMD being introduced in 1997, use of AMD has not increased
Deaths in the ICU • More patients died in the hospitals and ICUs than at home 2 decades ago • Approx. 65% of Americans die in hospitals • Withdrawal and withholding of therapy of life support are the most common causes of deaths in the ICU
Reasons for aggressive Rx for dying patients • Lack of training among doctors and nurses in the clinical aspects of withdrawing life support • Problems in communication
NMEC Recommendation in July 1995 Legislation in Advanced Medical Directives (AMDS) is required to provide patients with the legal means to continue to exercise autonomy over their medical treatment even when they are incompetent and in the final stages of their terminal illness.
Advanced Medical Directives Act • Passed in Parliament in May 1996 • An Act to provide for, and give legal effect • to, medical practitioners against artificial • prolongation of the dying process and for matters • connected therewith
Surgical ICU - Singapore General Hospital Guidelines on withholding/withdrawal of therapy and “Do Not Resuscitate” Order were adopted in 1996
Audit of 2,431Admission to Surgical Intensive Care Unit, Singapore General Hospital BL Lim. YW Chan Ann Acad Med Singapore 1998;27:314-7
The Practice of Forgoing Life Support in the Critically Ill ‘Old Old’: A Singapore Perspective IYO Leong, DYH Tai Ann Acad Med Singapore 2001;30:260-4
Forgoing Life Support (FLS) therapy Total 282 patients57 with FLS Orders (20.2%)
1st draft of DNR Guidelines was presented at a Clinical Heads of Departments Meeting in 1998. • Main concerns were Selection Criteria and Medico-Legal implications.
The draft was amended almost 10 times with clinicians and hospital legal advisors’ input. • Final draft was presented and accepted at the Clinical Heads of Departments Meeting on 15 March 2000.
Definition • Resuscitation - standard CPR with • full cardiac, • pharmacologic and • respiratory intervention • DNR - No CPR when cardiorespiratory arrest occurs
Patients who may be considered for DNR • Death would be imminent • Application of extra-ordinary life-sustaining treatment • would only serve to postpone the moment of death • Medical futility
Guidelines for ordering DNR • Only Consultant or Associate Consultant in-charge is allowed • to initiate • Patient’s condition fulfills DNR criteria • MEDICAL CONSENSUS - at least 3 doctors, • two of whom must be a specialists • DNR must be documented clearly with date, time and names of • persons involved
Participants and Process • DNR order should be discussed with the patient and • family members while patient is competent. • For comatose or mentally incompetent patients, • decisions will be guided by their AMD • DNR is a professional decision • Any disputes can be referred to SGH Bioethics Committee
SGH Bioethics Committee Appointed by Medical Board on 15 May 2000 to review guidelines for end-of-life issues
DNR Order • DNR order should lead to discussion and decision about • intensive care, ventilatory support, dialysis, and medication • Abandonment of the patient must neither occur nor be perceived • DNR order must be reviewed daily as part of the usual ongoing • evaluation for patient and revoked if patient’s condition improves
Useful “Test” Questions • What is right for patient ? • What does patient wish ? • What is “Standard” therapy ? • What would Peers & Experts do ? • What would I wish if I were the patients ? • If the patients were my spouse, child, parent, friend etc ? • What is lawful ?
Costs • Diagnosis-Related Groups (DRGs) • Charges for care delivered exceeded income received • Net revenue loss of US$24,098 for class IV • Therapeutic Intervention Scoring System • Reimbursement for Intensive Care Services under DRGs • C Bekes, S Fleming, E Scott. Crit Care Med 1988; 16:478
Economics of dying • 1992: US ICUs accounted for 1%GDP (62 billion) • 30% of patients admitted to MICU/SICU fell into a potentially ineffective category,ie. resource consumption in the upper 25th percentile and survival of less than 100 days • Potentially ineffective care is delivered less often to Medicare patients enrolled in HMO than to those in traditional fee-for-service health plans
Challenges • Patient • Relatives • Medical/nursing staff
Patient • The biggest challenge is none of them has AMD • They are not sophisticated enough to understand the implications of AMD • Cultural taboos to talk about dying issues • Most are quite ignorant on terminal illness
Family members • Guilt feelings • Reluctant to reveal diagnosis to patient • Always request for best to be given to the patient even if the chances of recovery are remote and costs of therapy are high • The most unreasonable relatives are usually those who never took care of the patients • Family conference with all family members, primary physicians, intensivists & ICU nurse.
Medical staff • Not trained to communicate bad news • Difficulties in obtaining consensus • Education for Physicians on End-of-life Care (EPEC)
Conclusion • Good medicine treats a person, rather than a condition. • Respect for the dignity of person requires that they neither • be under-treated nor over-treated, but rather have access to • whatever care is appropriate to their condition.