Download
1 / 66
660 likes | 681 Vues
Explore the biology, microbiology, virology, and immunology of the Picornavirus family, focusing on the pathogenesis of enterovirus infection, replication in different tissues, and clinical syndromes associated with specific genera. Learn about the reclassification of certain Coxsackie and Echo viruses and the properties of enteroviruses. Dive into the specifics of Poliomyelitis, its types, morphology, cultivation, resistance, and pathogenesis. Discover the clinical findings of Poliovirus infection, including asymptomatic illness, aseptic meningitis, and paralytic Poliomyelitis.

E N D
Picornavirus Family Medical biology, microbiology, virology, immunology department By as. E.V. Pokryshko
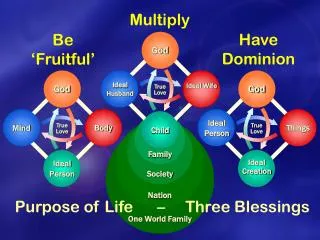
Pathogenesis of enterovirus infection Replication in oropharynx Rhino,echo, coxsackie,polio Primary viremia Secondary viremia Target Tissue Skin Muscle Brain Meninges Liver Echo Coxsackie A Echo Coxsackie A, B Polio Coxsackie Echo Polio Coxsackie Echo Coxsackie
* Reclassification of coxsackievirus A23 as echovirus 9, echovirus 8 as 1, echovirus 10 as reovirus, echovirus 28 as rhinovirus type 1A, and echovirus 34 as coxsackievirus A24.
POLIOMYELITIS • “Picornavirus” • 3 types: Poliovirus 1,2,3 • Ingested, spread by alimentary route: Commoner in areas of poor sanitation • Infants protected by maternal antibodies
Poliomyelitis is an acute infectious disease that in its serious form affects the central nervous system. The destruction of motor neurons in the spinal cord results in flaccid paralysis (less than 0.1%). However, most poliovirus infections are subclinical. Duringepidemic outbreaks, type I is most frequently isolated (in 65-95 per cent of cases) while types II and III account for the remaining 5-35 per cent of cases.
Morphology. The virus is 30 nm in size and forms intranuclear inclusions. The virion is icosahedral and consists ofa single sense-strand RNA and a protein capsid containing 32 spherical subunits (capsomeres). This genome RNA serves as an mRNA and initiates the synthesis of virus macromolecules. The poliomyelitis virus has neither an outer membrane nor lipids and is therefore not sensitive to the effect of ether and sodium desoxycholate.
Cultivation. SPE. The poliomyelitis virus is cultivated on kidney cells of green African monkeys and on diploid human cells devoid of latent SV40 viruses. The cytopathic effect is attended by destruction and the formation of granules in the infected cells.
Resistance. The virus is extremely resistant to photodynamic inactivation. It survives in sterile water at room temperature for a period of more than 100 days, in milk for 90 days, in faeces in the cold for more than 6 months, and in sewage for several months. It withstands exposure to 0.5-1 per cent phenol solutions and remains viable for several weeks at pH 3.8-8.5. The poliomyelitis virus is sensitive to calcium chlorate lime, chloramine, formalin, potassium permanganate, and hydrogen peroxide solutions. It is rapidly killed on boiling.
Pathogenesis • Source of infection:Apparent and subclinical patients • Incubation:is usually 7-14 days, but it may rangefrom 3 to 35 days.
Transmission • Fecal – oral route: poor hygiene, dirty diapers (especially in day-care settings) • Ingestion via contaminated food and water • Contact with infected hands • Inhalation of infectious aerosols
Pathogenesis 1. The mouth is the portal of entry of the virus. 2. The virus first multiplies in the tonsils, the lymph nodes of the neck, Peyer's patches, and the small intestine. The virus is regularly present in the throat and in the stools before the onset of illness. One week after onset there is little virus in the throat, but virus continues to be excreted in the stools for several weeks, even though high antibody levels are present in the blood. 3. Viremia The virus may be found in the blood of patients with abortive and nonparalytic poliomyelitis. 4. The central nervous system may then be invaded by way of the circulating blood.
Pathogenesis Poliovirus can spread along axons of peripheral nerves to the central nervous system, and there it continues to progress along the fibers of the lower motor neurons to increasingly involve the spinal cord or the brain. Poliovirus invades certain types of nerve cells, and in the process of its intracellular multiplication it may damage or completely destroy these cells. The anterior horn cells of the spinal cord are most prominently involved, but in severe cases the intermediate gray ganglia and even the posterior horn and dorsal root ganglia are often involved. In the brain, the reticular formation, vestibular nuclei, and deep cerebellar nuclei are most often affected. The cortex is virtually spared, with the exception of the motor cortex along the precentral gyms.
Clinical Findings.When an individual susceptible to infection is exposed to the virus, one of the following responses may occur: • inapparent infection without symptoms (asymptomatic illness), the minor illness – 90% infected people • aseptic meningitis – 1%-2% of patients with poliovirus infections, • paralytic poliomyelitis, the major illness0.1% to 2% of persons with poliovirus • Only about 1% of infections are recognized clinically.
Abortive Poliomyelitis. This is the commonest form of the disease. The patient has only the minor illness, characterized by fever, malaise, drowsiness, headache, nausea, vomiting, constipation, and sore throat in various combinations. The patient recovers in a few days. The diagnosis of abortive poliomyelitis can be made only when the virus is isolated or antibody development is measured.
Nonparalytic Poliomyelitis (Aseptic Meningitis).In addition to the above symptoms and signs, the patient with the nonparalytic form presents stiffness and pain in the back and neck. The disease lasts 2-10 days, and recovery is rapid and complete. In a small percentage of cases, the disease advances to paralysis.
Paralytic Poliomyelitis. The major illness usually follows the minor illness described above, but it may occur without the antecedent first phase. The predominating complaint is flaccid paralysis resulting from lower motor neuron damage. The maximal recovery usually occurs within 6 months, with residual paralysis lasting much longer.
Immunity sIgA and neutralizing antibody (IgG, IgA, IgM) persist for life span • Immunity is permanent to the type causing the infection. There may be a low degree of heterotypic resistance induced by infection, especially between type 1 and type 2 polioviruses. • Passive immunity is transferred from mother to offspring. The maternal antibodies gradually disappear during the first 6 months of life. Passively administered antibody lasts only 3-5 weeks.
Lab Diagnosis • Definitive diagnosis is made by osolation of the virus from stool, CFS, oropharyngeal secretions • Cell culture involves fibroblastic MRC-5 cells CPE is usually evident within 36 hours • Serotyping is based on neutralization of CPE by standardized antisera using intersecting pool followed by specific sera. • ELISA • IFA • neutralizing Test • CFT
Treatment There is no specific treatment. Treatment involves reduction of pain and muscle spasm and maintenance of respiration and hydration. When the fever subsides, early mobilization and active exercise are begun. There is no role for antiserum. Early injections of gamma-globulin, blood transfusion, wide use of vitamins C and B,-, amino acids (leucine, glutamic acid), analgesics (analgine, amidopyrine, pantopon, etc.), mediators, and stimulants (proserine, galanthamine, dibazol, etc.) are recommended. An orthopaedic regimen is set up from the first day that paralysis develops to prevent contractures and deformations, and exercise therapy is carried out during the rehabilitation period. An apparatus for artificial respiration is employed when there are respiration disturbances.
Prevention Both oral polio vaccine (OPV live, attenuated, Sabin, 1957) and inactivated poliovirus vaccine (IPV, Salk, 1954) are avilable IPV is used for adult immunization and Immunocopromised patients
Both killed and live virus vaccines induce antibodies and protect the central nervous system from subsequent invasion by wild virus. Low levels of antibody resulting from killed vaccine have little effect on intestinal carriage of virus. The gut develops a far greater degree of resistance after live virus vaccine, which seems to be dependent on the extent of initial vaccine virus multiplication in the alimentary tract rather than on serum antibody level.
Advantages and disadvantages of OPV Advantages • Effectiveness • Lifelong immunity • Induction of secretory antibody response similar to that of natural infection • Possibility of attenuated virus circulating in community by spread to contacts (indirect immunization)(herd immunity) • Ease of administration • Lack of need for repeated boosters
Advantages and disadvantages of OPV Disadvantages • Risk of vaccine-associated poliomyelites in vaccine recipients or contacts • Spread of vaccine to contacts without their consent • Unsafe administration for immunodeficient patients
Advantages and disadvantages of IPV Advantages • Effectiveness • Good stability during transport and in storage • Safe administration in immunodeficient patients • No risk of vaccine-related disease
Advantages and disadvantages of IPV Disadvantages • Lack of induction of local (gut) immunity • Need for booster vaccine for lifelong immunity • Fact that injection is more painful than oral administration • Fact that higher community immunization levels are needed than with live vaccine
COXSACKIEVIRUSES The coxsackieviruses comprise a large subgroup of the enteroviruses. They produce a variety of illnesses in human beings, including aseptic meningitis, herpangina, pleurodynia, hand, foot, and mouth disease, myo- and pericarditis, common colds, and possibly diabetes. Coxsackieviruses have been divided into 2 groups, A and B, having different pathogenic potentials for mice.
Group A viruses produce widespread myositis in the skeletal muscles of newborn mice, resulting in flaccid paralysis without other observable lesions. Group Bviruses may produce spasticity effect insucking mice,focal myositis, encephalitis, and, most typically, necrotizing steatitis involving mainly fetal fat lobules. Some B strains also produce pancreatitis, myocarditis, endocarditis, and hepatitis in both suckling and adult mice. Normal adult mice tolerate infections with group B coxsackieviruses.
Herpangina: There is an abrupt onset of fever, sore throat, anorexia, dysphagia, vomiting, or abdominal pain. The pharynx is usually hyperaemic, and characteristic discrete vesicles occur on the anterior pillars of the fauces, the palate, uvula, tonsils, or tongue. The illness is self-limited and most frequent in small children.
Hand, Foot, and Mouth Disease: The syndrome is characterized by oral and pharyngeal ulcerations and a vesicular rash of the palms and soles that may spread to the arms and legs. Vesicles heal without crusting, which clinically differentiates them from the vesicles of herpes- and pox-viruses. The rare deaths are caused by pneumonia.
Hand-foot-and-mouth disease • Hand-foot-and-mouth disease: mostly coxackie A • fever, malaise, sore throat, vesicles on bucсal mucosa, tongue, hands, feet, buttocks • highly infectious • resolution – 1w
ECHOVIRUSES The echoviruses (enteric cytopathogenic human orphan viruses) are grouped together because they infect the human enteric tract and because they can be recovered from humans only by inoculation of certain tissue cultures. Over 30 serotypes are known, but not all cause human illness. Aseptic meningitis, febrile illnesses with or without rash, common colds, and acute hemorrhagic conjunctivitis are among the diseases caused by echoviruses. Properties of the Viruses General Properties. Echoviruses are typical enteroviruses measuring 24-30 nm.
Important Characteristics • Not produce diseases in sucking mice, rabbits, or monkeys; • Cause aseptic meningitis, infantile diarrhea, • Monkey kidney and human embryonated kidney cell culture