Download
1 / 65
760 likes | 1.86k Vues
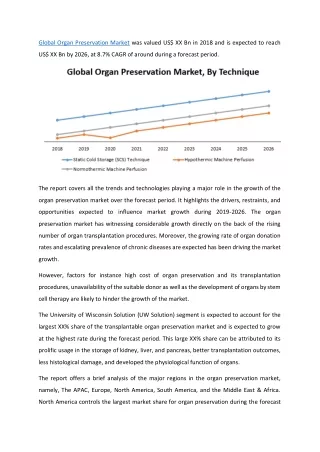
Organ Preservation with Histidine-Tryptophan-Ketoglutarate (HTK) Solution Clinical Results. Bijan Eghtesad, M.D. John J. Fung, M.D. Ph.D. Department of General Surgery Cleveland Clinic. Orlando, 5/19/2007. Organ Preservation. P RESERVATIVE S OLUTIONS. Organ Preservation.

E N D
Organ Preservation with Histidine-Tryptophan-Ketoglutarate (HTK) Solution Clinical Results Bijan Eghtesad, M.D. John J. Fung, M.D. Ph.D. Department of General Surgery Cleveland Clinic Orlando, 5/19/2007
Organ Preservation PRESERVATIVE SOLUTIONS
Organ Preservation Preservation solutions are used to maintain the organ in optimal condition from the time of explantation until transplantation
Organ Preservation Preservation offers four major advantages to a transplant program • Time to transport the organ • Time to allow tissue matching • Time to prepare the recipient and surgical team • Quality of organ function; better postop recovery
Organ Preservation Principles of organ preservation : • Provide for hypothermia • Prevent cellular swelling • Avoid biochemical injury
History of Organ Preservation • Simple cooling with cold solution • Continuous hypothermic perfusion • Collins (1967) • Euro-Collins (1980) • University of Wisconsin - ViaSpan (1986) • HTK - Custodiol (1980’s) • Celsior – 1994 • Polysol • Normothermic perfusion
Component Eurocollins UW HTK Celsior Sodium (mmol/L) 10 40 15 100 Potassium (mmol/L) 107 120 10 15 Magnesium( mmol/L) - 5 4 13 Calcium (mmol/L) - - 0.015 0.25 Sulfate (mmol/L) - 5 - - Lactobionate (mmol/L) - 100 - 80 Phosphate (mmol/L) 57 25 - - Raffinose (mmol/L) - 30 - - Adenosine (mmol/L) - 5 - - Glutathione (mmol/L) - 3 - 3 Allopurinol (mmol/L) - 1 - - Ketoglutarate/Glutamic Acid (mmol/L) - - 1 20 Histidine (mmol/L) - - 198 30 Starch (gm/L) - 50 - - Mannitol (mmol/L) - - 30 60 Glucose (mmol/L) 194 - - - Tryptophan (mmol/L) - - 2 - Osmolality (mOsm/L) 355 320 310
UW Solution •Significance of impermeant molecules in preventing cell swelling • First developed for and applied in preservation of canine pancreas • Impermeants lactobionate and raffinose prevent cell swelling • Hydroxyethyl starch to minimize interstitial edema during machine perfusion, not necessary during storage
UW Solution • Glutathione as antioxidant •Adenosine as precursor for energy metabolism •Allopurinol as free-radical scavenger •Phosphate buffer • High [K+], low [Na+]
UW Solution: Disadvantages • Glutathione is oxidized during storage: addition of fresh GSH immediately before use; other additives • High viscosity • Solution cannot be released into circulation (high K content) • Huge particles ~ 100 µm in diameter contained in original solution: must use in-line filtration with 40 µm pore size • Particles caught in capillary bed of perfused organ, resulting in vascular constriction, impeded reperfusion, and reduction of functional recovery
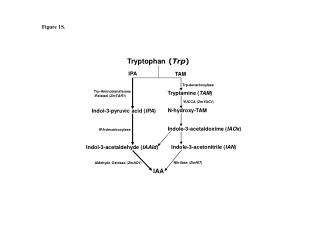
M.M. Gebhard, H.J. Kirlum, C. Schlegel. Organ preservation with the solution HTK
HTK Solution (Custodiol) • Decrease in [Na+] to 1/10 of normal and [Ca++] to 1/100 normal is optimal to fix resting potential of cell in the polarized or minimally depolarized state • Mannitol: • Metabolically inert • Does not ‘infiltrate’ into the cell by special transport system • Acts as oxygen radical scavenger
HTK Solution (Custodiol) • Ideal Buffer: • Well tolerated and capable of being broken down by the body • Good penetration from intravascular to interstitial space • Low penetration intracellularly to avoid edema • Histidine & histidine HCl provide substantial buffering capacity • Doubles buffering capacity of the transplanted organ, slowing down the pH drop •Buffer system better able to moderate damaging pH reductions even during phases of higher storage temperatures
HTK Solution (Custodiol) • No colloid • Viscosity equal to that of pure water from 1 to 350C, with mean flow rate 3X that of UW solution at equal perfusion pressure • Organs cool down to lower temperatures more rapidly than with UW • Tryptophan as membrane stabilizer • Ketoglutarate as energy substrate •One solution for preservation of all organs
Kidney Transplantation • de Boer et al: Eurotransplant randomized multicenter kidney graft preservation study comparing HTK with UW and Euro-collins. Transplant Int, 1999, 12:447 • UW (168) vs EC (155) vs HTK (336), • DGF: 33% UW vs 43% EC* vs 31% HTK • 3-year Graft survival: UW (68%), HTK (73%), EC (67%) • Conclusions: HTK is comparable to UW in its preservative capabilities in cadaveric renal transplantation Factors influencing DGF: Donor age, cause of death, CIT
J. De Boer, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK, UW and Euro-Collins (Transplant Int, 1999)
J. De Boer, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK, UW and Euro-Collins (Transplant Int, 1999)
Liver Transplantation • Hatano et al: Hepatic preservation with histidine-tryptophan-ketoglutarate solution in living-related and cadaveric liver transplantation. Clinical Science (1997), 93:81 • Evaluated graft oxygenation state after reperfusion in LRLT using near-infrared (NIR) tissue spectroscopy • LRD liver: HTK (15) vs. UW (49) • CAD liver: HTK (30) vs. UW (18)
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997) LRLT Intraoperative changes in mean value of oxygen saturation of Hb at 10 points in liver graft After reflow of operation
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997) LRLT CV of oxygen saturation of Hb at 10 points in liver graft, indicating heterogeneity of tissue oxygenation After reflow of operation
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997) Cadaveric Intraoperative changes in mean value of hepatic tissue oxygen saturation of Hb at 10 points in liver graft
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997)
E. Hatano, et al. Tissue oxygenation in living related liver transplantation (Clinical Science, 1997)
Biliary Complications Develop up to 30% of Patients After Liver Transplantation
Post-liver Transplant Biliary Strictures • Biliary strictures after liver transplantation: 10-30% • Adequate flushing of peri-biliary arterial tree is important • High viscosity preservation solutions might not completely flush the small donor peri-biliary plexus
Peri-Biliary Vascular Plexus Alpini et al.
Pirenne et al. Liver Transplantation, 7:540-545, 2001 Two group of liver recipients: Group 1 (24): Donor aortic flush with Marshall solution Portal vein with UW Group 2 (27): Donor aortic flush with UW Portal vein with UW Similar Donor age, local vs. imported, split/full liver, incidence of multiple vessels in the donor, indication for OLTX, recipient age, T-tube vs. no T-tube, Post OLTX peak ALT/AST, immunosuppressive regimen and treatment for rejection. CIT: 692+190 ( group 1) vs. 535+129, (group 2), (P=.001) Preservation cost 1.9 times greater in the UW than in the Marshall group
Pirenne et al. Liver Transplantation, 7:540-545, 2001 • Recipient surgeon : Same surgeon • All biliary reconstruction duct-to-duct except in one patient • One-year patient and graft survival 92% (1) and 100% (2) • Biliary stricture: 1/24 (4.1%) group 1 8/27 (29.2%) group 2 Biliary stricture in group 1: 4 months after LTX and anastomotic Biliary strictures in group 2: 1-12 months after LTX and anastomotic, extrahepatic, intrahepatic or a combination of intra-and extrahepatic
Background Hannover (1988-2000) 1068 patients HTK (461) UW (607) PF 439 478 PNF 22(4.8%) 29 (4.8%) CIT > 15 hrs: Comparable PF (5.6%) vs. PNF (7.1%) Comparable biliary complication rate Comparable graft and patient survival University of Gottingen (2002) 134 transplants HTK (63) UW (71) Similar graft function Increased rate of intrahepatic ischemic type biliary strictures in UW group Essen/Chicago (Live donor liver transplantation, 2002) 30 patients HTK (15) UW (15) Comparable biochemical values, patient and graft survival
University of Pittsburgh Pilot Study on HTK Experience with LDLT 2001
Liver Transplantation, Live Donor HTK/UW # Lobe AST1 AST7 ALT1 ALT7 Outcome 1 LLS 388 76 318 35 Good LLS 1530 222 984 457 Good 2 LLS 318 32 218 81 Good LLS 212 21 156 38 Good 3 RL 1134 54 1146 271 Re-OLTX, 3 mos (Good) RL 1783 58 1569 465 Good 4 RL 491 33 313 67 Good RL 271 174 177 152 Good 5 LL 719 70 514 84 Re-OLTX, 3 wks (Good) LL 541 46 256 79 Good 6 RL 749 31 790 66 Good RL 1972 50 1969 247 Died (Sepsis, 3 months) 7 RL 216 55 157 82 Good RL 236 39 143 105 Good
Pittsburgh Protocol • Trial of HTK in 100 consecutive standard multiorgan donors - comparison group to be historic (UW) age matched controls (2:1) for age, CIT, organs removed and transplanted using CORE donor database. Outcomes to include: • Patient and graft survival • Initial function vs. DGF vs. PNF • HTK to be used on all NHBD and liver alone donors
Patients HTK UW Donors 84 169 Gender 49 M, 35 F 98 M, 71 F Age 2 Wks - 75Y 3Y - 75Y (47) (46) (43.3 + 19) (43.7 + 18.8) Recipients Gender 62 M, 22 F 101 M, 68 F Age 2Y - 71Y 1Y - 73Y (50) (52) (49.7 + 13) (50.3 + 12.3)
Primary Liver Disease HTK UW 84(%) 169(%) Hepatitis C 35(41) 58(34) Alcohol 14(16) 23(14) PSC 7(8) 15(9) PBC 5(5) 7(4) Hepatitis B 4(5) 5(3) FHF 0(0) 4(2) Others 17(20) 42(25) Re-OLTX 4(5) 14(8)
Liver Transplantation, CadavericUW / HTK Age D/R 43.7+18.8 (3-75) / 50.3+12.3 (1-73) Age D/R 43.3+19 (1wk-75) / 49.7+13 (2-71) CIT 619+191 CIT 616+193 AST1 1293+2907 Median: (597) (97-31490) AST1 1489.2+2404 (595) (72-15750) ALT1 834.9+1192 (483) (91-6552) ALT1 914.8+1131.3 (450) (85-7016) AST7 99.9+189.2 (51) (17-1969) AST7 72.9+64.4 (55) (12-498) ALT7 189.4+191.2 (137) (40-1408) ALT7 178.9+145.6 (139) (22-568)
Graft Function HTK UW 84 (%) 169 (%) IGF 66 (78.5) 134 (79) DGF 16 (19) 15 (9) PNF 2 (2.2) 20 (11.8) CIT > 14 hours 13 (%) 27 (%) IGF 8 (62) 19 (70) DGF 3 (23) 5 (18.5) PNF 2 (15) 3 (11)
30-day Survival HTK UW 84 169 Graft 94% 83% Patient 96% 89% Re-OLTX 3 13 in 30 days HAT 2 4
Long-term Biliary Complications(one year) HTK UW (76) (134) Anastomotic stricture 3 5 Diffuse (ischemic) stricture 0 2 Bile leak 1 1
Non-Heart-Beating Donors HTK UW 8 15 IGF 8 12 PNF 0 3 Biliary complications 1 3 Anastomotic 1 1 Diffuse 0 1 Bile leak 0 1
HTK vs. UWCadaveric liver Transplantation Mangus et. al. Liver Transplantation 2006;12:226-230 Indiana University Retrospective study. 7/2002 – 12/2004 378 Patients UWHTK 204 174 CIT (hrs) 3-20 (7.0) 3-13 (7.0) PNF 1.5% 0.5% 30-day mortality 14 (7%) 12 (7%) 1-year Patient survival 84.6% 82.1% 1-year Graft survival 81.7% 80.8% Biochemical values the same except higher bilirubin in the first 14 days in HTK group Preservation solution volume: 3200 + 1400 3800 + 1000 Cost saving/donor: $422 OPO with 160 donors/year: $67520
HTK vs. UW in LDLT Chan et. al. Liver Transplantation 2004; 10:1415-1421 (Hong Kong) UWHTK Number of patients 30 30 Age 38.5 35.5 CIT 112 (79 + 334) 111.5 (75 + 222) Biliary stricture* 10 (33%) 6 (20%) Pre-reperfusion flush Yes No Graft loss 0 1 Hospital mortality 0 0 Biochemicals: Same, except PT (higher in HTK) Cost analysis: UW $137.6 higher than HTK/patient * Not significant
HTK vs. UW in LDLTA Prospective Study Testa et. al. Liver Transplantation 2003; 9:822-826 (Chicago and Essen) Donors: Right lobe Age: (33 + 10) 18 M, 12 F Recipients: Age: (49 + 9), 20 M, 10 F, MELD: 13.4 + 7.4 Mean Follow-up 13 + 7 months UWHTK Perfusion solution 14 16 Artery 1 mL/g 3 mL/g Portal vein 1 mL/g 1.5 mL/g Pre-reperfusion flush Yes No (practical advantage) CIT 147 + 44 144 + 40 Patient survival 79% 88% Graft survival 72% 83% PNF 1 0 HAT 1 1 Liver biochemical values: Similar No intrahepatic biliary stricture Overall: Equally effective. HTK has practical and economical advantage
HTK solution for organ preservation in human liver transplantationA prospective multi-center observation study Pokorny et. al. Transplant International 2004; 17:256-260 (Austria, Germany) 214 patients in 4 European centers (1996-1999) 5 liters of HTK for preservation CIT 444 + 224 All vascular anastomoses completed before reperfusion No pre-reperfusion flush PNF 2.3%, Initial dysfunction 6.5% Graft dysfunction not correlated with CIT 1-year patient and graft survival 83% and 80% (unrelated to CIT) HTK: safe and effective and easy to use. Comparable to UW with less cost.
HTK vs. UW in liver transplantationA meta-analysis Feng et.al. Unpublished data (in press)
HTK vs. UW in liver transplantation A meta-analysis P= 0.87 RR 1.01 Patient Survival P= 0.86 RR 1.01 Graft Survival Feng et.al. Unpublished data (in press)