Download
1 / 1
10 likes | 138 Vues
This study investigates the differences in plaque morphology and burden between South Asian men and women using coronary computed tomography angiography. It highlights that men exhibit a higher incidence of non-calcified plaque and a lower occurrence of mixed plaque compared to women, despite similar total plaque burden. Additionally, men are more likely to have diabetes and dyslipidemia. Findings suggest that gender may influence plaque characteristics among South Asians, warranting further longitudinal studies to assess its impact on coronary artery disease presentations.

E N D
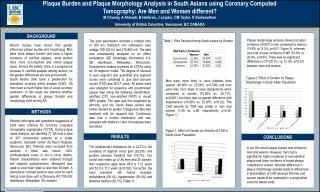
Plaque Burden and Plaque Morphology Analysis in South Asians using Coronary Computed Tomography: Are Men and Women different? M Chandy, A Ahmadi, B Heilbron, J Leipsic, CM Taylor, K Ramanathan University of British Columbia, Vancouver, BC CANADA BACKGROUND Plaque morphology analysis showed a higher incidence of NCP in men compared to women (19.6% vs. 8.3%, p=0.01, Figure 3), whereas men had a lower incidence of MP (10.8% vs. 20.0%, p=0.04). There was no significant difference in CP (20.1%, vs. 12.0%, p=0.23) between men and women. Table 1: Risk Factors Among South Asians by Gender The scan parameters included a rotation time of 350 ms, 64x0.625 mm collimation, tube voltage 100-120 kV, and 275-800 mA. The data was subsequently analyzed on an offline workstation (GE Advantage Workstation 4.4, GE Healthcare, Milwaukee, Wisconsin). Experienced readers reviewed all CCTAs using an 18 segment model. The degree of stenosis in each segment was quantified and segment scores were combined to give total stenosis scores (TSS) and SCCT score. All scans were also analyzed for presence and predominant plaque type using the following classification: calcified (CP), non-calcified (NCP) or mixed (MP) plaque. The data was first organized by ethnicity, and the South Asian subset was further divided by gender. Categorical data was analyzed with chi squared test. Continuous data had a normal distribution and was analyzed with student’s t test. All analyses were two tailed. Recent studies have shown that gender influences plaque burden and morphology. Men have more plaque burden and have a higher incidence of calcified plaques, while women have more non-calcified and mixed plaque types. Among the elderly, there is a progressive increase in calcified plaques among women, so the gender differences are less pronounced. South Asians (SA) have a predilection for premature coronary artery disease (CAD). SA men have a much higher rate of acute coronary syndrome. In this study, we examine whether gender differences in plaque burden and morphology exist among SA. Figure 2: Effect of Gender on Plaque Morphology in South Asian Population Men were more likely to have diabetes than women (30.00% vs. 22.58%, p=0.006) and men were also more likely to have dyslipidemia when compared to women (75.00% vs. 38.71%, p=0.001), but there was no gender difference with hypertension (45.00% vs. 32.26%, p=0.22). The CAD severity by TSS was similar in men and women (1.48 vs. 0.80, respectively; p=0.36, Figure 1). METHODS Patients with signs and symptoms suggestive of CAD were referred for coronary computed tomography angiography (CCTA). Using unique name analysis, we identified 71 SA from a total of 327 consecutive patients at a single academic Canadian center (St Paul’s Hospital, Vancouver, BC). Patients were excluded from analysis if there was known CAD, uninterpretable scans or not in sinus rhythm. Patient characteristics were obtained through self reported questionnaires. Metoprolol was used to slow heart rates to less than 65 bpm. A dual phase contrast protocol was used for each helical scan done with a Discovery HD 750 (GE Healthcare, Milwaukee, WI) scanner. Figure 1: Effect of Gender on Severity of CAD in South Asian Population RESULTS CONCLUSIONS The predominant indications for a CCTA in SA consisted of atypical chest pain (62.0%) and positive exercise treadmill test (19.7%). Our cohort was made up of 46 men and 25 women; their respective ages were 48.9 ± 11.2 years and 52.0 ± 11.2 years (p=0.392). For all SA, the most prevalent risk factors included: dyslipidemia (59.1%), hypertension (39.4%) and diabetes mellitus (26.7%) (Table 1). In our SA cohort plaque burden was similar for men and women. However, men had a significantly higher incidence of non-calcified plaque and lower incidence of mixed plaque compared to women. Whether difference in plaque morphology actually leads to differences in presentation of CAD amongst SA men and women needs to be evaluated in a longitudinal outcome based study. * University of British Columbia, Vancouver, BC Canada





















